Department of Epidemiology and Biostatistics, School of Public Health, Peking University, Beijing, China.
Medical Informatics Center, Peking University, Beijing, China.
J Cachexia Sarcopenia Muscle. 2023 Apr;14(2):1075-1082. doi: 10.1002/jcsm.13197. Epub 2023 Feb 28.
The associations of multimorbidity patterns with transitions between frailty states remain unclear in older individuals.
We used data from the National Health and Aging Trends Study 2011-2019. Frailty was measured annually using the Fried frailty phenotype. Multimorbidity patterns at baseline were identified using latent class analysis based on 14 chronic conditions. We used the semi-Markov multi-state model to investigate the influences of multimorbidity characterized by condition counts and patterns on subsequent frailty transitions over follow-ups.
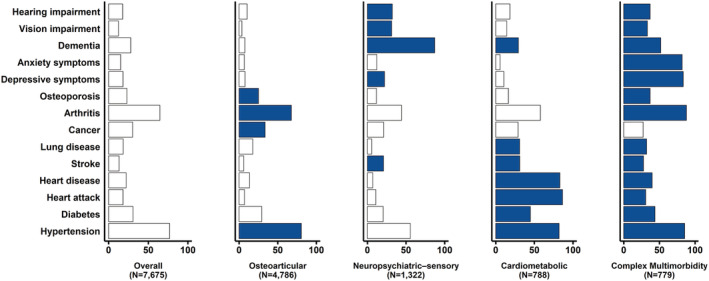
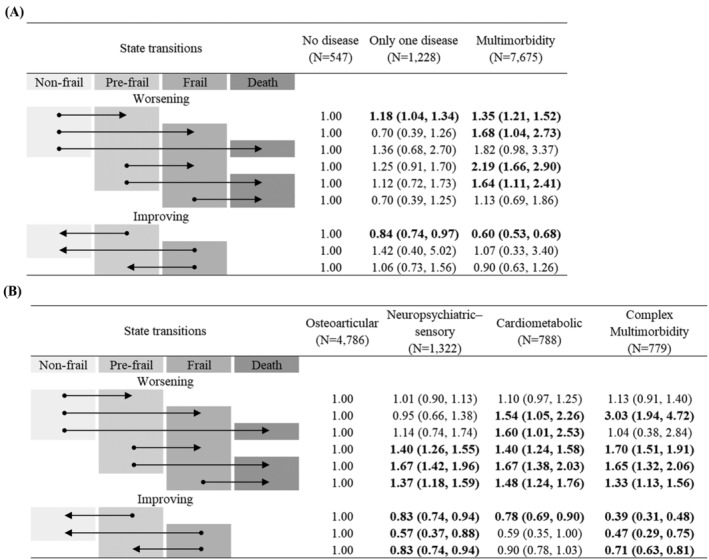
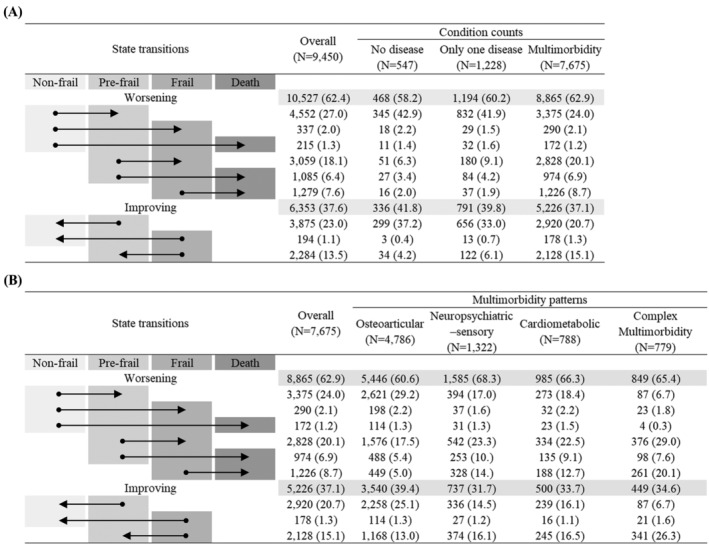
Among 9450 participants aged ≥65 years at baseline, 34.8% were non-frail, 48.1% were pre-frail and 17.0% were frail. Over a median follow-up of 4.0 years, 16 880 frailty transitions were observed, with 10 527 worsening and 6353 improving. For 7675 participants with multimorbidity, four multimorbidity patterns were identified: osteoarticular pattern (62.4%), neuropsychiatric-sensory pattern (17.2%), cardiometabolic pattern (10.3%) and complex multimorbidity pattern (10.1%). Compared with no disease, multimorbidity was significantly associated with an increased risk of worsening transitions, including from non-frail to pre-frail (hazard ratio [HR] = 1.35; 95% confidence interval [CI] = 1.21-1.52), from non-frail to frail (HR = 1.68; 95% CI = 1.04-2.73), from pre-frail to frail (HR = 2.19; 95% CI = 1.66-2.90) and from pre-frail to death (HR = 1.64; 95% CI = 1.11-2.41). Compared with the osteoarticular pattern, neuropsychiatric-sensory, cardiometabolic and complex multimorbidity patterns had a significantly higher risk of worsening frailty (all P < 0.05).
Multimorbidity was associated with dynamic transitions between frailty states and death among older American adults, and the associations varied across multimorbidity patterns. The findings could offer significant implications for public health policymakers in planning interventions and healthcare resources. They also might inform clinicians regarding providing targeted clinical treatment and health management based on multimorbidity patterns of older people.
多种疾病模式与老年人虚弱状态之间的转变关系仍不清楚。
我们使用了 2011 年至 2019 年国家健康老龄化趋势研究的数据。每年使用 Fried 虚弱表型来衡量虚弱。根据 14 种慢性疾病,采用潜在类别分析来确定基线时的多种疾病模式。我们使用半马尔可夫多状态模型来研究以疾病数量和模式为特征的多种疾病对随后随访中虚弱状态转变的影响。
在 9450 名年龄≥65 岁的基线参与者中,34.8%是非虚弱的,48.1%是虚弱前期的,17.0%是虚弱的。在中位数为 4.0 年的随访中,观察到 16880 次虚弱状态转变,其中 10527 次恶化,6353 次改善。对于 7675 名有多种疾病的参与者,确定了四种多种疾病模式:骨关节炎模式(62.4%)、神经精神感觉模式(17.2%)、心脏代谢模式(10.3%)和复杂多种疾病模式(10.1%)。与无疾病相比,多种疾病与恶化转变的风险增加显著相关,包括从不虚弱到虚弱前期(风险比 [HR]1.35;95%置信区间 [CI]1.21-1.52),从不虚弱到虚弱(HR1.68;95%CI1.04-2.73),从虚弱前期到虚弱(HR2.19;95%CI1.66-2.90)和从虚弱前期到死亡(HR1.64;95%CI1.11-2.41)。与骨关节炎模式相比,神经精神感觉、心脏代谢和复杂多种疾病模式与虚弱恶化的风险显著增加(均 P<0.05)。
多种疾病与美国老年人虚弱状态和死亡之间的动态转变有关,且关联因多种疾病模式而异。研究结果可为公共卫生政策制定者规划干预措施和医疗保健资源提供重要意义。这些结果还可能为临床医生根据老年人的多种疾病模式提供有针对性的临床治疗和健康管理提供信息。