Ruers Theo, Van Coevorden Frits, Punt Cornelis J A, Pierie Jean-Pierre E N, Borel-Rinkes Inne, Ledermann Jonathan A, Poston Graeme, Bechstein Wolf, Lentz Marie-Ange, Mauer Murielle, Folprecht Gunnar, Van Cutsem Eric, Ducreux Michel, Nordlinger Bernard
Netherlands Cancer Institute, Antoni Van Leeuwenhoek Ziekenhuis, Amsterdam, The Netherlands.
Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands.
J Natl Cancer Inst. 2017 Sep 1;109(9). doi: 10.1093/jnci/djx015.
Tumor ablation is often employed for unresectable colorectal liver metastases. However, no survival benefit has ever been demonstrated in prospective randomized studies. Here, we investigate the long-term benefits of such an aggressive approach.
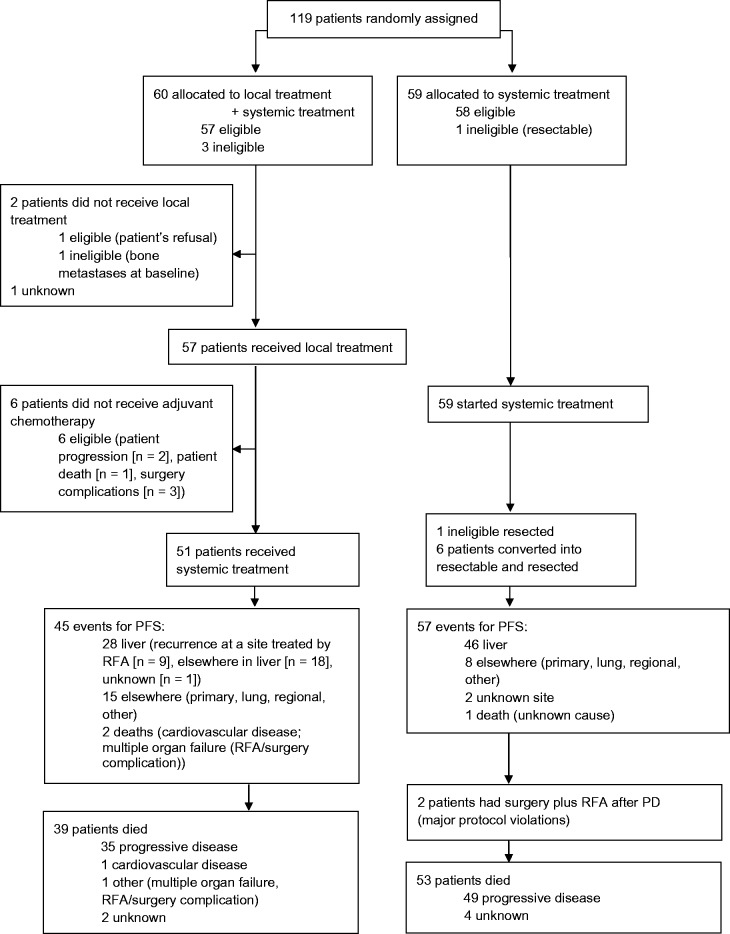
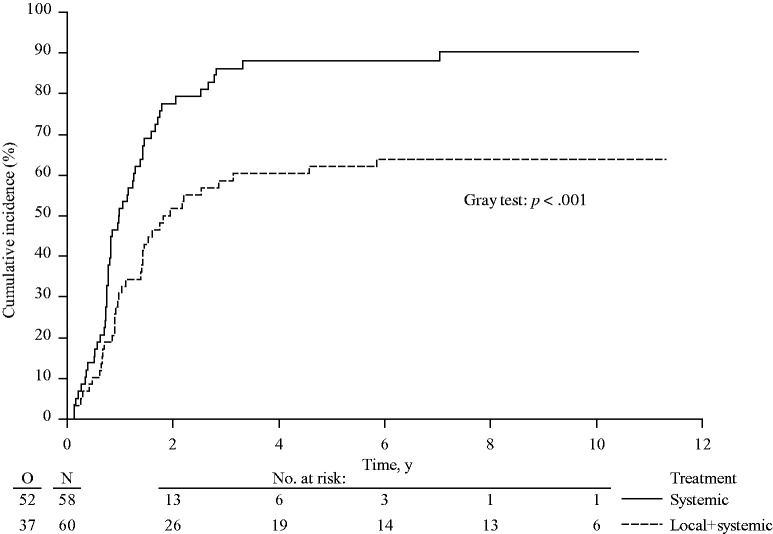
In this randomized phase II trial, 119 patients with unresectable colorectal liver metastases (n < 10 and no extrahepatic disease) received systemic treatment alone or systemic treatment plus aggressive local treatment by radiofrequency ablation ± resection. Previously, we reported that the primary end point (30-month overall survival [OS] > 38%) was met. We now report on long-term OS results. All statistical tests were two-sided. The analyses were according to intention to treat.
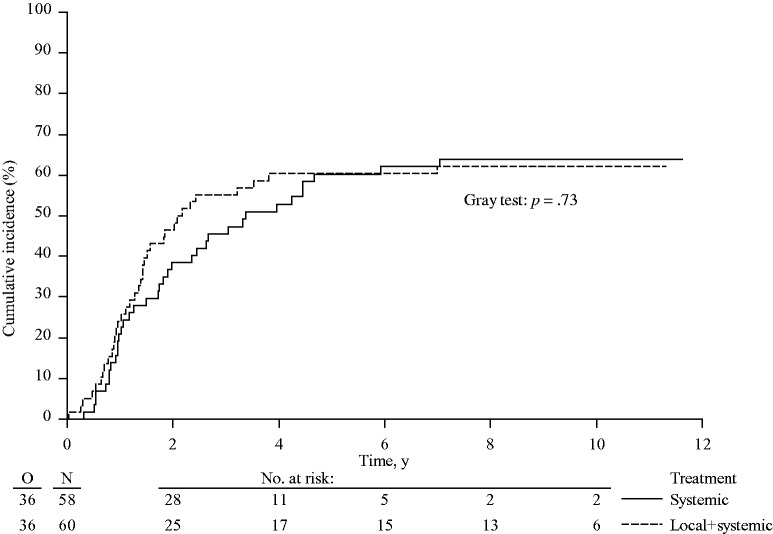
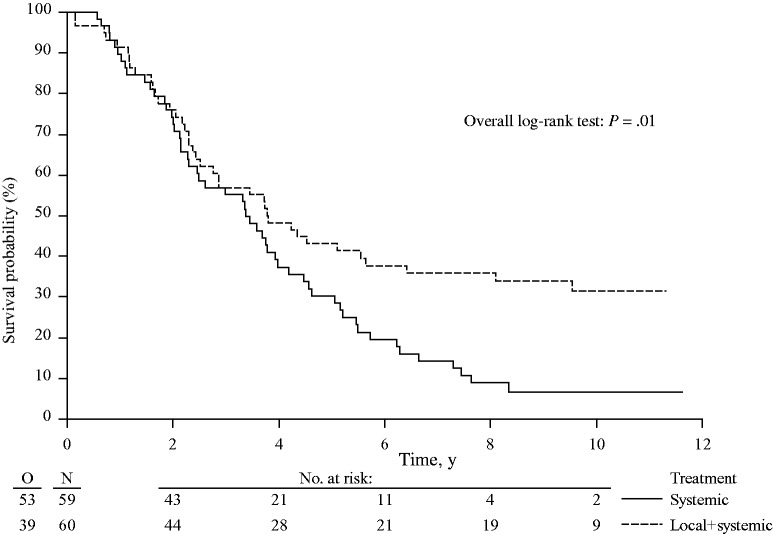
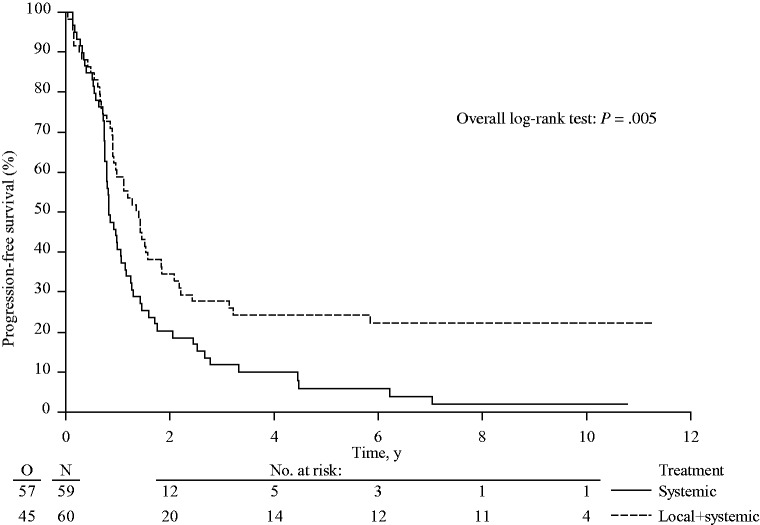
At a median follow up of 9.7 years, 92 of 119 (77.3%) patients had died: 39 of 60 (65.0%) in the combined modality arm and 53 of 59 (89.8%) in the systemic treatment arm. Almost all patients died of progressive disease (35 patients in the combined modality arm, 49 patients in the systemic treatment arm). There was a statistically significant difference in OS in favor of the combined modality arm (hazard ratio [HR] = 0.58, 95% confidence interval [CI] = 0.38 to 0.88, P = .01). Three-, five-, and eight-year OS were 56.9% (95% CI = 43.3% to 68.5%), 43.1% (95% CI = 30.3% to 55.3%), 35.9% (95% CI = 23.8% to 48.2%), respectively, in the combined modality arm and 55.2% (95% CI = 41.6% to 66.9%), 30.3% (95% CI = 19.0% to 42.4%), 8.9% (95% CI = 3.3% to 18.1%), respectively, in the systemic treatment arm. Median OS was 45.6 months (95% CI = 30.3 to 67.8 months) in the combined modality arm vs 40.5 months (95% CI = 27.5 to 47.7 months) in the systemic treatment arm.
This phase II trial is the first randomized study demonstrating that aggressive local treatment can prolong OS in patients with unresectable colorectal liver metastases.
肿瘤消融术常用于无法切除的结直肠癌肝转移患者。然而,前瞻性随机研究从未证明其能带来生存获益。在此,我们研究这种积极治疗方法的长期益处。
在这项随机II期试验中,119例无法切除的结直肠癌肝转移患者(转移灶数量<10个且无肝外疾病)接受单纯全身治疗或全身治疗加射频消融±切除的积极局部治疗。此前,我们报告主要终点(30个月总生存率[OS]>38%)已达到。我们现在报告长期OS结果。所有统计检验均为双侧检验。分析按照意向性治疗原则进行。
中位随访9.7年,119例患者中有92例(77.3%)死亡:联合治疗组60例中有39例(65.0%),全身治疗组59例中有53例(89.8%)。几乎所有患者死于疾病进展(联合治疗组35例,全身治疗组49例)。联合治疗组的OS有统计学显著差异(风险比[HR]=0.58,95%置信区间[CI]=0.38至0.88,P=0.01)。联合治疗组的3年、5年和8年总生存率分别为56.9%(95%CI=43.3%至68.5%)、43.1%(95%CI=30.3%至55.3%)、35.9%(95%CI=23.8%至48.2%),全身治疗组分别为55.2%(95%CI=41.6%至66.9%)、30.3%(95%CI=19.0%至42.4%)、8.9%(95%CI=3.3%至18.1%)。联合治疗组的中位OS为45.6个月(95%CI=30.3至67.8个月),全身治疗组为40.5个月(95%CI=27.5至47.7个月)。
这项II期试验是第一项随机研究,表明积极的局部治疗可延长无法切除的结直肠癌肝转移患者的总生存期。