Division of Digestive and Liver Diseases, Department of Medicine, Columbia University Medical Center, 630 West 168th Street, New York, NY, 10032, USA.
Department of Medicine, Columbia University Medical Center, New York, USA.
Intensive Care Med. 2018 Aug;44(8):1203-1211. doi: 10.1007/s00134-018-5268-8. Epub 2018 Jun 23.
Loss of colonization resistance within the gastrointestinal microbiome facilitates the expansion of pathogens and has been associated with death and infection in select populations. We tested whether gut microbiome features at the time of intensive care unit (ICU) admission predict death or infection.
This was a prospective cohort study of medical ICU adults. Rectal surveillance swabs were performed at admission, selectively cultured for vancomycin-resistant Enterococcus (VRE), and assessed using 16S rRNA gene sequencing. Patients were followed for 30 days for death or culture-proven bacterial infection.
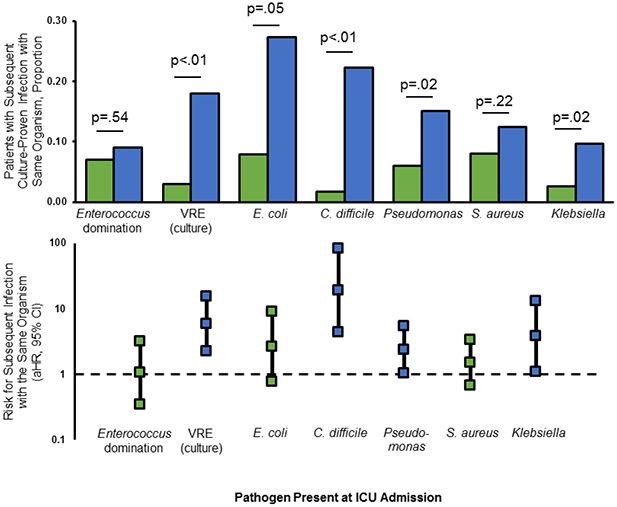
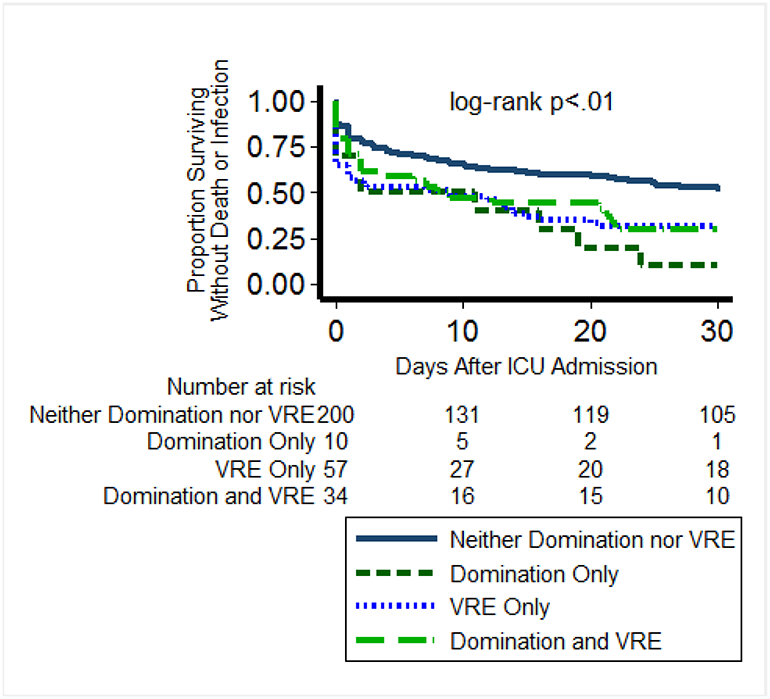
Of 301 patients, 123 (41%) developed culture-proven infections and 76 (25%) died. Fecal biodiversity (Shannon index) did not differ based on death or infection (p = 0.49). The presence of specific pathogens at ICU admission was associated with subsequent infection with the same organism for Escherichia coli, Pseudomonas spp., Klebsiella spp., and Clostridium difficile, and VRE at admission was associated with subsequent Enterococcus infection. In a multivariable model adjusting for severity of illness, VRE colonization and Enterococcus domination (≥ 30% 16S reads) were both associated with death or all-cause infection (aHR 1.46, 95% CI 1.06-2.00 and aHR 1.47, 95% CI 1.00-2.19, respectively); among patients without VRE colonization, Enterococcus domination was associated with excess risk of death or infection (aHR 2.13, 95% CI 1.06-4.29).
Enterococcus status at ICU admission was associated with risk for death or all-cause infection, and rectal carriage of common ICU pathogens predicted specific infections. The gastrointestinal microbiome may have a role in risk stratification and early diagnosis of ICU infections.
胃肠道微生物组内定植抵抗力的丧失促进了病原体的扩张,并与某些人群的死亡和感染有关。我们检测了重症监护病房(ICU)入院时的肠道微生物组特征是否可预测死亡或感染。
这是一项对成人 ICU 进行的前瞻性队列研究。在入院时进行直肠监测拭子采集,选择性地对万古霉素耐药肠球菌(VRE)进行培养,并使用 16S rRNA 基因测序进行评估。患者在 30 天内接受死亡或培养阳性细菌感染的随访。
在 301 名患者中,123 名(41%)发生了培养阳性感染,76 名(25%)死亡。粪便生物多样性(Shannon 指数)与死亡或感染无关(p=0.49)。在 ICU 入院时存在特定病原体与随后感染相同病原体有关,如大肠杆菌、铜绿假单胞菌、克雷伯菌和艰难梭菌,而 VRE 入院与随后的肠球菌感染有关。在调整疾病严重程度的多变量模型中,VRE 定植和肠球菌优势(≥16S 读数的 30%)均与死亡或全因感染相关(aHR 1.46,95%CI 1.06-2.00 和 aHR 1.47,95%CI 1.00-2.19);在没有 VRE 定植的患者中,肠球菌优势与死亡或感染的风险增加相关(aHR 2.13,95%CI 1.06-4.29)。
ICU 入院时肠球菌状态与死亡或全因感染风险相关,直肠携带常见 ICU 病原体可预测特定感染。胃肠道微生物组可能在 ICU 感染的风险分层和早期诊断中发挥作用。