OncoStem Diagnostics Private Limited, Bangalore, India.
Clinical Persona Inc, East Palo Alto, California.
Cancer Med. 2019 Apr;8(4):1755-1764. doi: 10.1002/cam4.2049. Epub 2019 Mar 7.
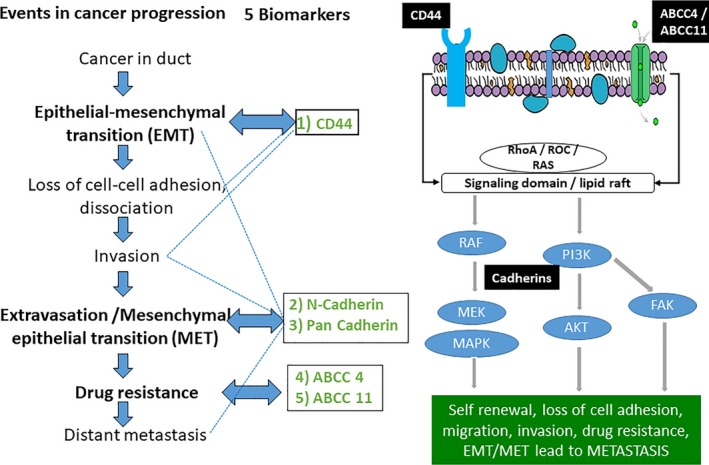
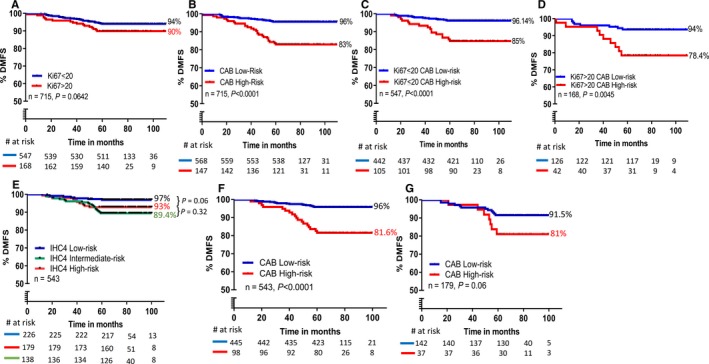
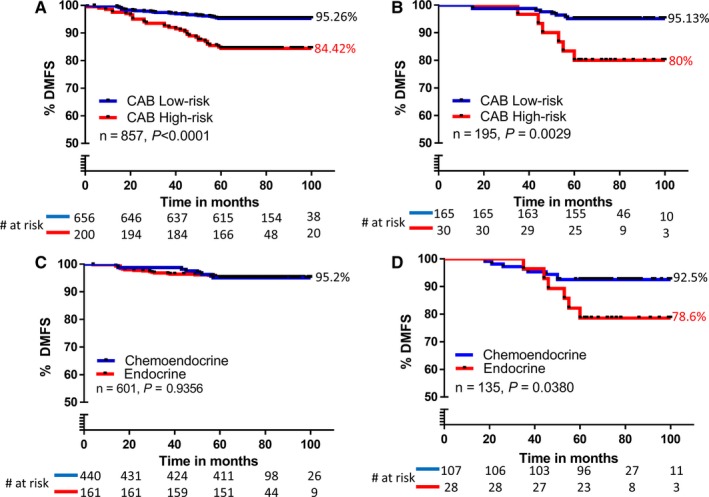
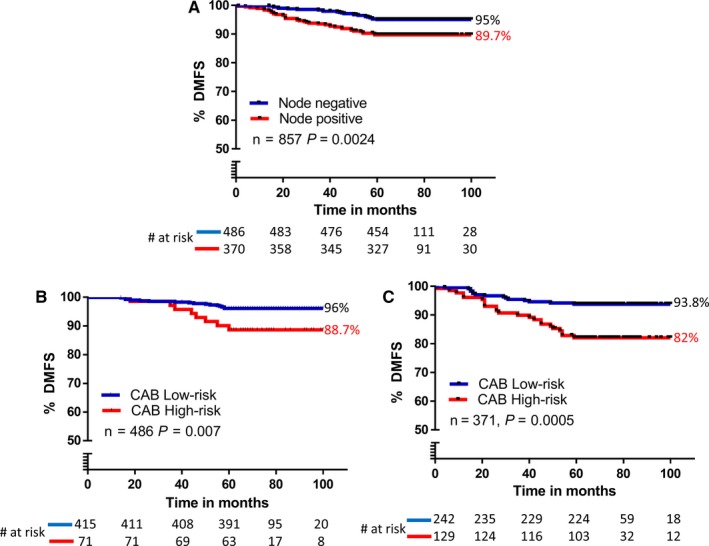
CanAssist-Breast (CAB) is an immunohistochemistry (IHC)-based prognostic test for early-stage Hormone Receptor (HR+)-positive breast cancer patients. CAB uses a Support Vector Machine (SVM) trained algorithm which utilizes expression levels of five biomarkers (CD44, ABCC4, ABCC11, N-Cadherin, and Pan-Cadherin) and three clinical parameters such as tumor size, grade, and node status as inputs to generate a risk score and categorizes patients as low- or high-risk for distant recurrence within 5 years of diagnosis. In this study, we present clinical validation of CAB. CAB was validated using a retrospective cohort of 857 patients. All patients were treated either with endocrine therapy or chemoendocrine therapy. Risk categorization by CAB was analyzed by calculating Distant Metastasis-Free Survival (DMFS) and recurrence rates using Kaplan-Meier survival curves. Multivariate analysis was performed to calculate Hazard ratios (HR) for CAB high-risk vs low-risk patients. The results showed that Distant Metastasis-Free Survival (DMFS) was significantly different (P-0.002) between low- (DMFS: 95%) and high-risk (DMFS: 80%) categories in the endocrine therapy treated alone subgroup (n = 195) as well as in the total cohort (n = 857, low-risk DMFS: 95%, high-risk DMFS: 84%, P < 0.0001). In addition, the segregation of the risk categories was significant (P = 0.0005) in node-positive patients, with a difference in DMFS of 12%. In multivariate analysis, CAB risk score was the most significant predictor of distant recurrence with hazard ratio of 3.2048 (P < 0.0001). CAB stratified patients into discrete risk categories with high statistical significance compared to Ki-67 and IHC4 score-based stratification. CAB stratified a higher percentage of the cohort (82%) as low-risk than IHC4 score (41.6%) and could re-stratify >74% of high Ki-67 and IHC4 score intermediate-risk zone patients into low-risk category. Overall the data suggest that CAB can effectively predict risk of distant recurrence with clear dichotomous high- or low-risk categorization.
CanAssist-Breast(CAB)是一种基于免疫组织化学(IHC)的早期激素受体(HR+)阳性乳腺癌患者的预后检测。CAB 使用支持向量机(SVM)训练算法,该算法利用五个生物标志物(CD44、ABCC4、ABCC11、N-钙粘蛋白和 Pan-钙粘蛋白)的表达水平以及肿瘤大小、分级和淋巴结状态等三个临床参数作为输入,生成风险评分,并将患者分为低风险或高风险,以在诊断后 5 年内发生远处复发的风险。在这项研究中,我们对 CAB 进行了临床验证。CAB 使用 857 例患者的回顾性队列进行验证。所有患者均接受内分泌治疗或化疗内分泌治疗。通过计算无远处转移生存(DMFS)和复发率的 Kaplan-Meier 生存曲线来分析 CAB 的风险分类。进行多变量分析以计算 CAB 高风险与低风险患者的风险比(HR)。结果表明,在单独接受内分泌治疗的亚组(n=195)和总队列(n=857,低风险 DMFS:95%,高风险 DMFS:80%)中,低风险(DMFS:95%)和高风险(DMFS:80%)类别之间无远处转移生存(DMFS)差异有统计学意义(P-0.002)。此外,风险类别的分离具有统计学意义(P=0.0005),在淋巴结阳性患者中,DMFS 差异为 12%。在多变量分析中,CAB 风险评分是远处复发的最显著预测因子,风险比为 3.2048(P<0.0001)。CAB 将患者分层为离散风险类别,与 Ki-67 和 IHC4 评分分层相比具有统计学意义。与 IHC4 评分(41.6%)相比,CAB 将队列中更高比例(82%)分类为低风险,并且可以将超过 74%的高 Ki-67 和 IHC4 评分中间风险区患者重新分类为低风险类别。总体而言,数据表明 CAB 可以有效预测远处复发的风险,具有明确的高低风险分类。