Mao David Weijia, Lee Yee Han Dave
Department of Orthopaedic Surgery, Changi General Hospital, Singapore.
Arthrosc Tech. 2020 Oct 22;9(10):e1541-e1545. doi: 10.1016/j.eats.2020.06.016. eCollection 2020 Oct.
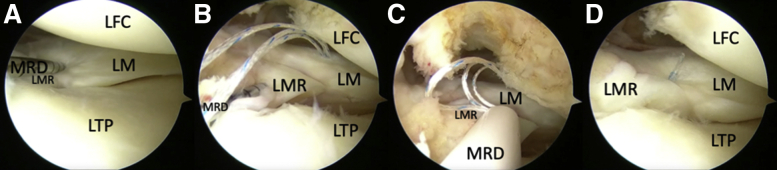
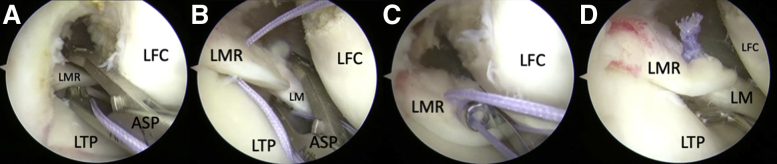
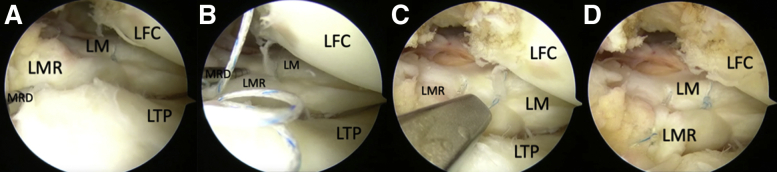
Meniscal radial root tears can disrupt the load-bearing function of the meniscus and worsen instability in anterior cruciate ligament-deficient knees. Paracentral radial tears adjacent to the root (types 1, 2, and 4) repaired with a transtibial pullout suture technique can lead to over-medialization of the meniscal root and a high-tension nonanatomic repair. We propose 2 all-inside techniques for anatomic repair of medial and lateral meniscal radial root tears with (1) an all-inside meniscal repair device and (2) an antegrade suture passer. We present the technical requirements and tips for these techniques. For lateral meniscal radial root repair with an all-inside meniscal repair device, ideal viewing is from an anterolateral portal with device entry from an anteromedial portal to reduce the risk of vascular injury. We recommend at least 2 stitches across the tear, with the depth setting limited to 18 to 20 mm for a central stitch and 16 mm or less for a peripherally placed stitch. For root repair with an antegrade suture passer, viewing should be from an anteromedial portal with the passer entering from an anterolateral portal. At least 2 stitches should be placed across the tear, with 1 central and 1 peripheral or 1 superior and 1 inferior.
半月板放射状根部撕裂会破坏半月板的承重功能,并加重前交叉韧带损伤膝关节的不稳定性。采用经胫骨拉出缝线技术修复的靠近根部的中央旁放射状撕裂(1型、2型和4型)可能导致半月板根部过度向内侧移位以及高张力非解剖修复。我们提出了两种全关节镜技术,用于内侧和外侧半月板放射状根部撕裂的解剖修复,(1)使用全关节镜半月板修复装置,(2)使用顺行缝线穿引器。我们介绍了这些技术的技术要求和技巧。对于使用全关节镜半月板修复装置进行外侧半月板放射状根部修复,理想的观察角度是从前外侧入路,装置从内侧前入路进入,以降低血管损伤风险。我们建议在撕裂处至少缝2针,中央缝线的深度设置限制在18至20毫米,周边缝线的深度设置在16毫米或更小。对于使用顺行缝线穿引器进行根部修复,观察应从前内侧入路,穿引器从外侧前入路进入。应在撕裂处至少放置2针缝线,1针中央和1针周边或1针上方和1针下方。