National Centre for Epidemiology and Population Health, Research School of Population Health, The Australian National University, 62 Mills Road, ACT, 2601, Acton, Australia.
BMC Med. 2021 Feb 17;19(1):50. doi: 10.1186/s12916-021-01934-5.
Following implementation of strong containment measures, several countries and regions have low detectable community transmission of COVID-19. We developed an efficient, rapid, and scalable surveillance strategy to detect remaining COVID-19 community cases through exhaustive identification of every active transmission chain. We identified measures to enable early detection and effective management of any reintroduction of transmission once containment measures are lifted to ensure strong containment measures do not require reinstatement.
We compared efficiency and sensitivity to detect community transmission chains through testing of the following: hospital cases; fever, cough and/or ARI testing at community/primary care; and asymptomatic testing; using surveillance evaluation methods and mathematical modelling, varying testing capacities, reproductive number (R) and weekly cumulative incidence of COVID-19 and non-COVID-19 respiratory symptoms using data from Australia. We assessed system requirements to identify all transmission chains and follow up all cases and primary contacts within each chain, per million population.
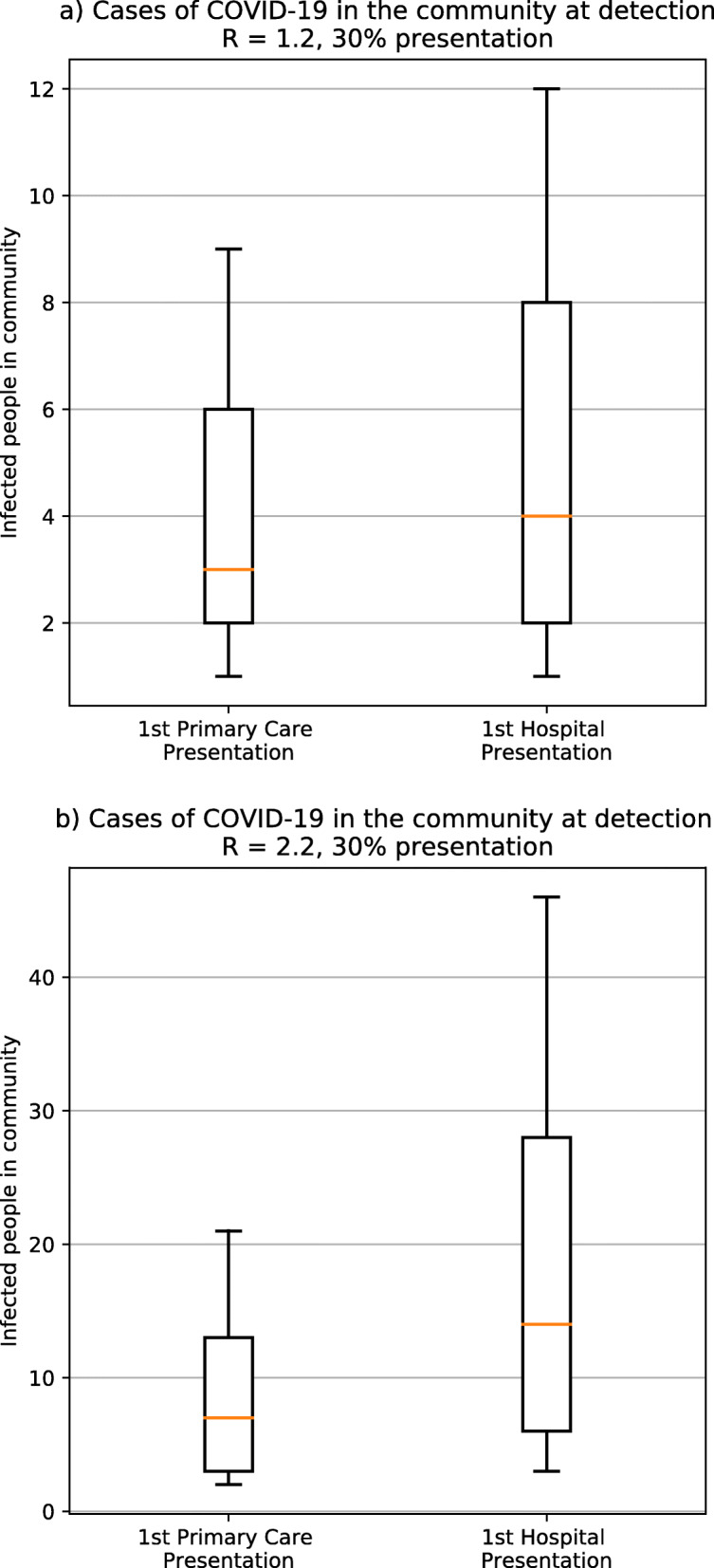
Assuming 20% of cases are asymptomatic and 30% of symptomatic COVID-19 cases present for testing, with R = 2.2, a median of 14 unrecognised community cases (8 infectious) occur when a transmission chain is identified through hospital surveillance versus 7 unrecognised cases (4 infectious) through community-based surveillance. The 7 unrecognised community upstream cases are estimated to generate a further 55-77 primary contacts requiring follow-up. The unrecognised community cases rise to 10 if 50% of cases are asymptomatic. Screening asymptomatic community members cannot exhaustively identify all cases under any of the scenarios assessed. The most important determinant of testing requirements for symptomatic screening is levels of non-COVID-19 respiratory illness. If 4% of the community have respiratory symptoms, and 1% of those with symptoms have COVID-19, exhaustive symptomatic screening requires approximately 11,600 tests/million population using 1/4 pooling, with 98% of cases detected (2% missed), given 99.9% sensitivity. Even with a drop in sensitivity to 70%, pooling was more effective at detecting cases than individual testing under all scenarios examined.
Screening all acute respiratory disease in the community, in combination with exhaustive and meticulous case and contact identification and management, enables appropriate early detection and elimination of COVID-19 community transmission. An important component is identification, testing, and management of all contacts, including upstream contacts (i.e. potential sources of infection for identified cases, and their related transmission chains). Pooling allows increased case detection when testing capacity is limited, even given reduced test sensitivity. Critical to the effectiveness of all aspects of surveillance is appropriate community engagement, messaging to optimise testing uptake and compliance with other measures.
在实施严格的遏制措施后,一些国家和地区的新冠病毒社区传播水平已很低。我们开发了一种高效、快速且可扩展的监测策略,通过彻底识别每个活跃的传播链,来检测剩余的新冠病毒社区病例。我们确定了措施,以便在解除遏制措施后,能够早期发现并有效管理任何传播的再次引入,从而确保无需重新实施严格的遏制措施。
我们通过以下方式比较了检测社区传播链的效率和灵敏度:医院病例;社区/初级保健的发热、咳嗽和/或急性呼吸道感染检测;以及无症状检测;使用监测评估方法和数学模型,根据澳大利亚的数据,改变检测能力、繁殖数(R)和每周新冠病毒和非新冠病毒呼吸道症状的累积发病率。我们评估了系统要求,以确定每百万人口中所有传播链,并对每个链中的所有病例和主要接触者进行随访。
假设 20%的病例为无症状,30%的有症状新冠病毒病例接受检测,R=2.2,与通过医院监测发现的 14 例未识别的社区病例(8 例传染性)相比,通过社区为基础的监测发现的 7 例未识别的社区病例(4 例传染性)。估计这 7 例未识别的社区上游病例会产生另外 55-77 名需要随访的主要接触者。如果 50%的病例为无症状,未识别的社区病例将增加到 10 例。在评估的任何情况下,对无症状社区成员进行筛查都无法彻底识别所有病例。对症状筛查的检测需求最重要的决定因素是非新冠病毒呼吸道疾病的水平。如果社区中有 4%的人有呼吸道症状,而这些症状中有 1%的人患有新冠病毒,那么使用 1/4 混合检测,需要大约 11600 次检测/百万人,具有 98%的病例检出率(2%漏检),灵敏度为 99.9%。即使灵敏度下降到 70%,在所有检查的情况下,与单独检测相比,混合检测更能有效发现病例。
对社区中所有急性呼吸道疾病进行筛查,并结合彻底和细致的病例和接触者识别和管理,能够及早发现并消除新冠病毒的社区传播。一个重要组成部分是识别、检测和管理所有接触者,包括上游接触者(即确定病例的潜在感染源及其相关传播链)。在检测能力有限的情况下,混合检测可以提高病例检出率,即使检测灵敏度降低。社区参与、优化检测率的信息传递以及遵守其他措施,对监测的所有方面的有效性至关重要。