VA Western New York Healthcare System, 3495 Bailey Avenue, Buffalo, NY, 14215, USA.
Division of Pulmonary, Critical Care, and Sleep Medicine, Department of Medicine, School of Medicine and Biomedical Sciences and School of Public Health and Health Professions, State University of New York at Buffalo, Buffalo, USA.
Intern Emerg Med. 2022 Apr;17(3):685-694. doi: 10.1007/s11739-021-02848-z. Epub 2021 Oct 12.
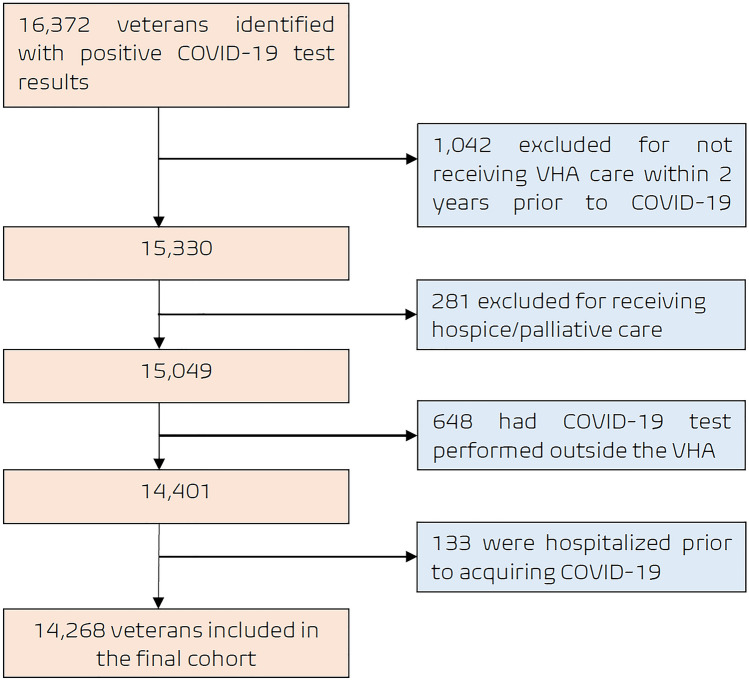
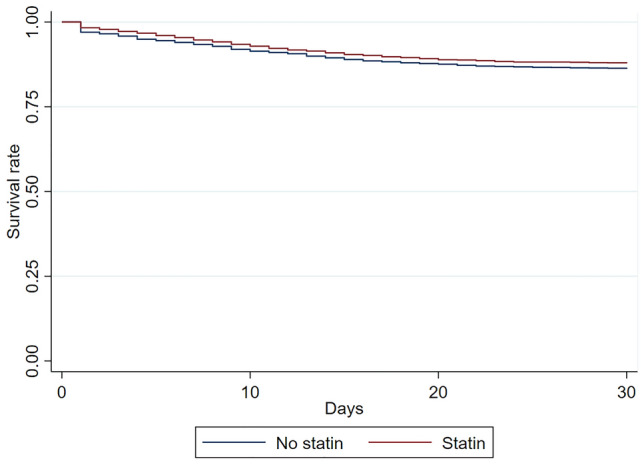
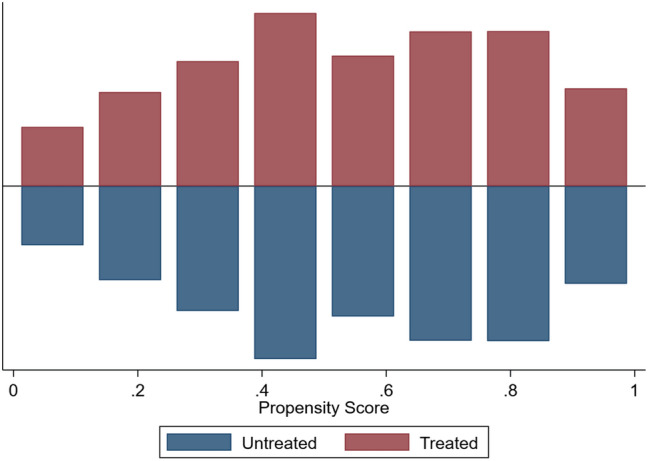
Statins have been advocated as a potential treatment for coronavirus disease-2019 (COVID-19) due to its pleotropic properties. The aim of the study was to elucidate the association between antecedent statin exposure and 30-day all-cause mortality, intensive care unit (ICU) admission and hypoxic respiratory failure requiring mechanical ventilation in patients diagnosed with COVID-19. Observational cohort study derived from the VA Corporate Data Warehouse of all veterans tested positive for COVID-19 between January 1st and May 31st, 2020. Antecedent use of statins was defined as a redeemed drug prescription in the 6 months prior to COVID-19 diagnosis. Propensity-matched mixed-effects logistic regression was performed, stratified by statin use. The study population comprised 14,268 patients with COVID-19 (median age 66 years (25th-75th percentile, 53-74), 90.7% men), of whom 7,168 were receiving a prescription for statins. Patients with statin exposure had a greater prevalence of comorbidities and a higher risk of mortality (Odd ratio [OR] 1.52; 95% confidence interval [CI] 1.37-1.68). After adjusting for covariates, statin exposure was not associated with a decreased mortality in the overall cohort by either Cox proportional hazards stratified model (HR 0.99; 95% CI 0.88-1.12) or propensity matching (HR .86; 95% CI 0.74-1.01). Similarly, there was no demonstrated advantage of statins in reducing the risk of ICU admission (HR 0.92; 95% CI 0.74-1.31) or hypoxic respiratory failure requiring mechanical ventilation (HR 1.02; 95% CI 0.81-1.29). Antecedent statin exposure in patients with COVID-19 was not associated with a decreased risk of 30-day all-cause mortality or need for mechanical ventilation.
由于其多效性,他汀类药物已被提倡作为治疗 2019 年冠状病毒病(COVID-19)的一种潜在疗法。本研究旨在阐明 COVID-19 患者中先前使用他汀类药物与 30 天全因死亡率、入住重症监护病房(ICU)和需要机械通气的低氧性呼吸衰竭之间的关联。这是一项从退伍军人事务部公司数据仓库中提取的观察性队列研究,研究对象为 2020 年 1 月 1 日至 5 月 31 日期间 COVID-19 检测呈阳性的所有退伍军人。先前使用他汀类药物定义为 COVID-19 诊断前 6 个月内 redeemed 的药物处方。采用倾向评分匹配的混合效应逻辑回归,按他汀类药物使用情况分层。该研究人群包括 14268 例 COVID-19 患者(中位年龄 66 岁(25 至 75 百分位数,53 至 74),90.7%为男性),其中 7168 例正在服用他汀类药物处方。暴露于他汀类药物的患者合并症患病率更高,死亡率风险更高(比值比 [OR] 1.52;95%置信区间 [CI] 1.37-1.68)。在校正协变量后,无论是 Cox 比例风险分层模型(HR 0.99;95%CI 0.88-1.12)还是倾向匹配(HR.86;95%CI 0.74-1.01),他汀类药物暴露均与全队列死亡率降低无关。同样,他汀类药物在降低 ICU 入院风险(HR 0.92;95%CI 0.74-1.31)或需要机械通气的低氧性呼吸衰竭风险(HR 1.02;95%CI 0.81-1.29)方面也没有显示出优势。COVID-19 患者先前使用他汀类药物与 30 天全因死亡率或机械通气需求降低无关。