Fiest Kirsten M, Krewulak Karla D, Makuk Kira, Jaworska Natalia, Hernández Laura, Bagshaw Sean M, Burns Karen E, Cook Deborah J, Doig Christopher J, Fox-Robichaud Alison, Fowler Robert A, Kho Michelle E, Parhar Ken Kuljit S, Rewa Oleksa G, Rochwerg Bram, Sept Bonnie G, Soo Andrea, Spence Sean, West Andrew, Stelfox Henry T, Parsons Leigh Jeanna
Department of Critical Care Medicine, Alberta Health Services & University of Calgary, Calgary, AB, Canada.
Department of Community Health Sciences & O'Brien Institute for Public Health, University of Calgary, Calgary, AB, Canada.
Crit Care Explor. 2021 Oct 25;3(10):e0562. doi: 10.1097/CCE.0000000000000562. eCollection 2021 Oct.
To create evidence-based consensus statements for restricted ICU visitation policies to support critically ill patients, families, and healthcare professionals during current and future pandemics.
Three rounds of a remote modified Delphi consensus process.
Online survey and virtual polling from February 2, 2021, to April 8, 2021.
Stakeholders (patients, families, clinicians, researchers, allied health professionals, decision-makers) admitted to or working in Canadian ICUs during the coronavirus disease 2019 pandemic.
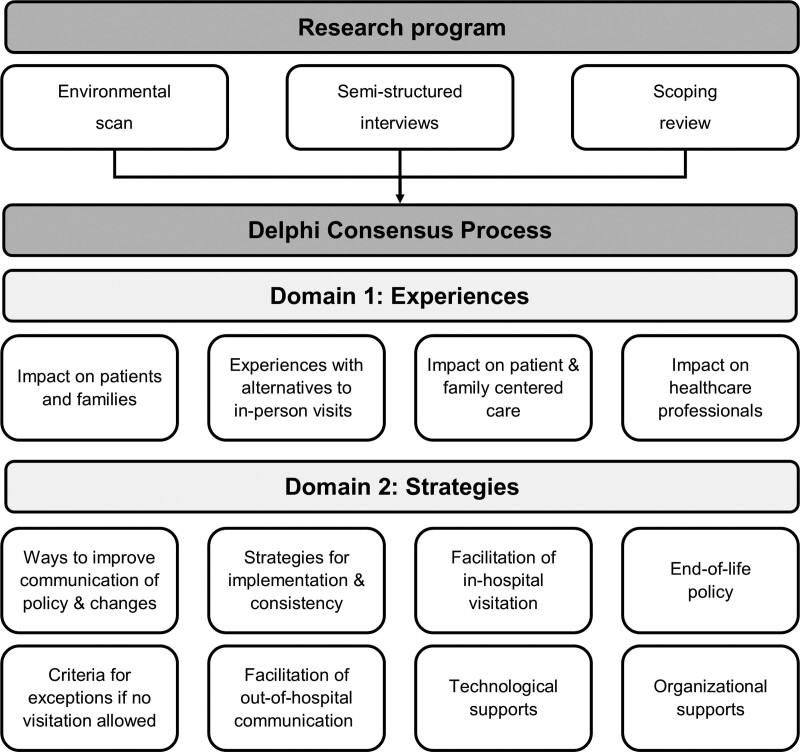
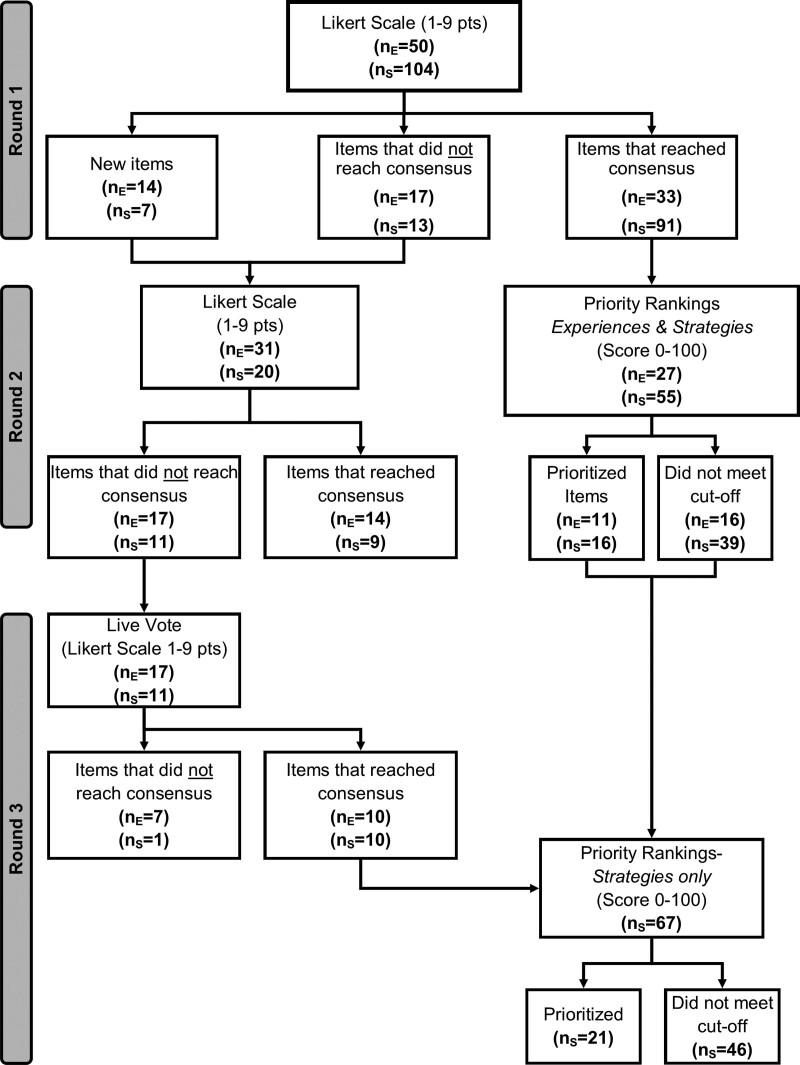
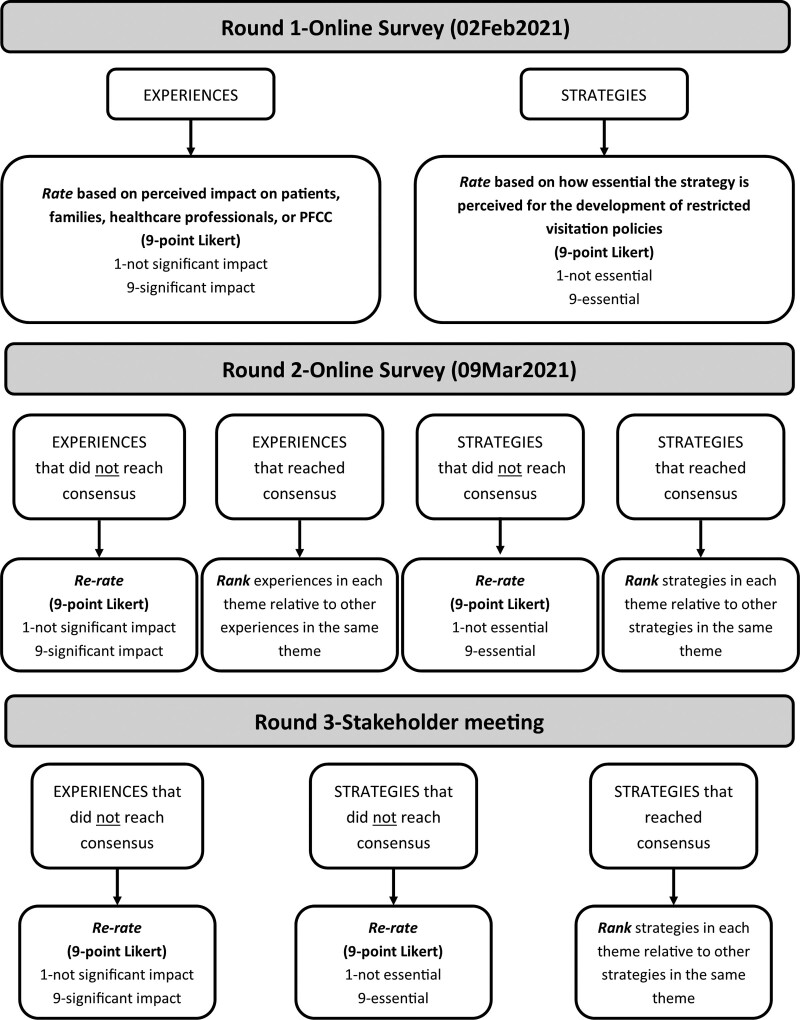
During Round 1, key stakeholders used a 9-point Likert scale to rate experiences (1-not significant, 9-significant impact on patients, families, healthcare professionals, or patient- and family-centered care) and strategies (1-not essential, 9-essential recommendation for inclusion in the development of restricted visitation policies) and used a free-text box to capture experiences/strategies we may have missed. Consensus was achieved if the median score was 7-9 or 1-3. During Round 2, participants used a 9-point Likert scale to re-rate experiences/strategies that did not meet consensus during Round 1 (median score of 4-6) and rate new items identified in Round 1. During Rounds 2 and 3, participants ranked items that reached consensus by order of importance (relative to other related items and experiences) using a weighted ranking system (0-100 points). Participants prioritized 11 experiences (e.g., variability of family's comfort with technology, healthcare professional moral distress) and developed 21 consensus statements (e.g., communicate policy changes to the hospital staff before the public, permit visitors at end-of-life regardless of coronavirus disease 2019 status, creating a clear definition for end-of-life) regarding restricted visitation policies.
We have formulated evidence-informed consensus statements regarding restricted visitation policies informed by diverse stakeholders, which could enhance patient- and family-centered care during a pandemic.
为制定基于证据的重症监护病房(ICU)探视限制政策的共识声明,以在当前及未来大流行期间为重症患者、家属和医护人员提供支持。
三轮远程改良德尔菲共识流程。
2021年2月2日至2021年4月8日的在线调查和虚拟投票。
在2019冠状病毒病大流行期间入住加拿大ICU或在其中工作的利益相关者(患者、家属、临床医生、研究人员、专职医疗人员、决策者)。
在第一轮中,关键利益相关者使用9点李克特量表对经历(1 - 无显著影响,9 - 对患者、家属、医护人员或以患者和家庭为中心的护理有显著影响)和策略(1 - 非必要,9 - 纳入探视限制政策制定的必要建议)进行评分,并使用自由文本框记录我们可能遗漏的经历/策略。如果中位数分数为7 - 9或1 - 3,则达成共识。在第二轮中,参与者使用9点李克特量表对第一轮中未达成共识的经历/策略(中位数分数为4 - 6)重新评分,并对第一轮中确定的新项目进行评分。在第二轮和第三轮中,参与者使用加权排序系统(0 - 100分)按重要性顺序(相对于其他相关项目和经历)对达成共识的项目进行排序。参与者对11种经历(例如,家属对技术的接受程度差异、医护人员的道德困扰)进行了优先排序,并就探视限制政策制定了21条共识声明(例如,在向公众公布之前向医院工作人员传达政策变化、无论2019冠状病毒病状况如何允许临终时的探视者、为临终制定明确的定义)。
我们制定了由不同利益相关者提供信息的、基于证据的关于探视限制政策的共识声明,这可以在大流行期间加强以患者和家庭为中心的护理。