Department of Physiology, Medical College of Wisconsin, Milwaukee, Wisconsin.
Cardiovascular Center, Medical College of Wisconsin, Milwaukee, Wisconsin.
Am J Physiol Renal Physiol. 2022 Jun 1;322(6):F639-F654. doi: 10.1152/ajprenal.00398.2021. Epub 2022 Apr 4.
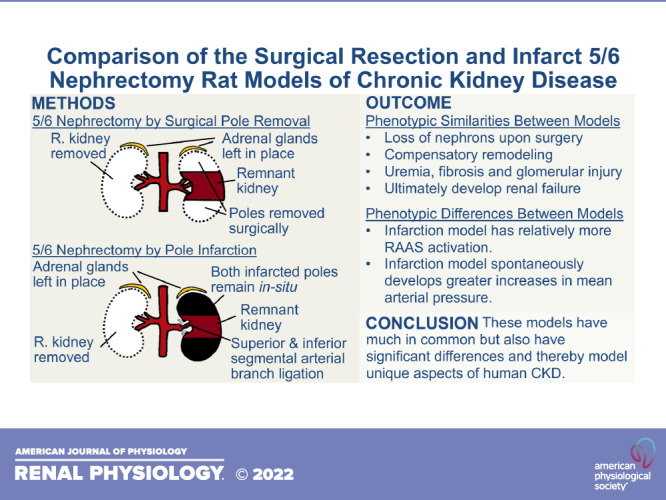
The 5/6 nephrectomy rat remnant kidney model is commonly used to study chronic kidney disease (CKD). This model requires the removal of one whole kidney and two-thirds of the other kidney. The two most common ways of producing the remnant kidney are surgical resection of poles, known as the polectomy model, or ligation of superior and inferior segmental renal arteries, resulting in pole infarction. These models have much in common, but also major phenotypic differences, and thus respectively model unique aspects of human CKD. The purpose of this review is to summarize phenotypic similarities and differences between these two models and their relation to human CKD while emphasizing their vascular phenotype. In this article, we review studies that have evaluated arterial blood pressure, the renin-angiotensin-aldosterone-system, autoregulation, nitric oxide, single-nephron physiology, angiogenic and antiangiogenic factors, and capillary rarefaction in these two models. In terms of phenotypic similarities, both models spontaneously develop hallmarks of human CKD including uremia, fibrosis, capillary rarefaction, and progressive renal function decline. They both undergo whole organ hypertrophy, hyperfiltration of functional nephrons, reduced renal expression of vascular endothelial growth factor, increased renal expression of antiangiogenic thrombospondin-1, impaired renal autoregulation, and abnormal vascular nitric oxide physiology. In terms of key phenotypic differences, the infarction model develops rapid-onset, moderate to severe systemic hypertension and the polectomy model develops early normotension followed by mild to moderate hypertension. Rats subjected to the infarction model have a markedly more active renin-angiotensin-aldosterone system. Comparison of these two models facilitates understanding of how they can be used for studying CKD pathophysiology.
5/6 肾切除大鼠残肾模型常用于研究慢性肾脏病(CKD)。该模型需要切除一个完整的肾脏和另一个肾脏的三分之二。产生残肾的两种最常见方法是切除极部,即极切除术模型,或结扎上下段肾动脉,导致极部梗死。这些模型有很多共同之处,但也有主要的表型差异,因此分别模拟了人类 CKD 的独特方面。本文的目的是总结这两种模型之间的表型相似性和差异及其与人类 CKD 的关系,同时强调其血管表型。在本文中,我们回顾了评估这两种模型的动脉血压、肾素-血管紧张素-醛固酮系统、自身调节、一氧化氮、单肾单位生理学、血管生成和抗血管生成因子以及毛细血管稀疏的研究。在表型相似性方面,两种模型均自发地表现出人类 CKD 的特征,包括尿毒症、纤维化、毛细血管稀疏和肾功能进行性下降。它们都经历整个器官肥大、功能性肾单位的高滤过、血管内皮生长因子的肾表达减少、抗血管生成的血小板反应蛋白-1 的肾表达增加、肾自身调节受损以及血管一氧化氮生理学异常。在关键表型差异方面,梗死模型发生快速发作的、中重度全身性高血压,而极切除术模型发生早期正常血压,随后发生轻度至中度高血压。接受梗死模型的大鼠的肾素-血管紧张素-醛固酮系统明显更为活跃。这两种模型的比较有助于理解它们如何用于研究 CKD 病理生理学。