Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York.
Division of Medical Oncology, Beth Israel Deaconess Medical Center, Dana-Farber/Harvard Cancer Center, Boston, Massachusetts.
Cancer. 2022 Jun 1;128(11):2085-2097. doi: 10.1002/cncr.34180. Epub 2022 Apr 5.
Conditional survival estimates provide critical prognostic information for patients with advanced renal cell carcinoma (aRCC). Efficacy, safety, and conditional survival outcomes were assessed in CheckMate 214 (ClinicalTrials.gov identifier NCT02231749) with a minimum follow-up of 5 years.
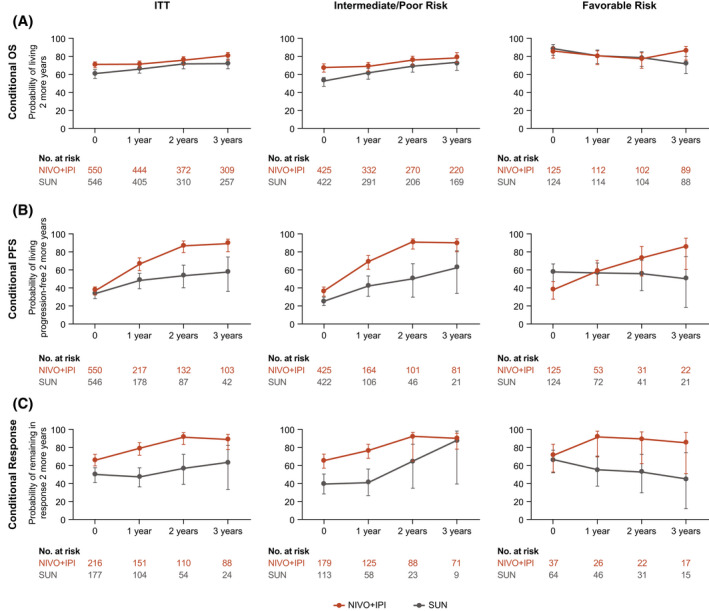
Patients with untreated aRCC were randomized to receive nivolumab (NIVO) (3 mg/kg) plus ipilimumab (IPI) (1 mg/kg) every 3 weeks for 4 cycles, then either NIVO monotherapy or sunitinib (SUN) (50 mg) daily (four 6-week cycles). Efficacy was assessed in intent-to-treat, International Metastatic Renal Cell Carcinoma Database Consortium intermediate-risk/poor-risk, and favorable-risk populations. Conditional survival outcomes (the probability of remaining alive, progression free, or in response 2 years beyond a specified landmark) were analyzed.
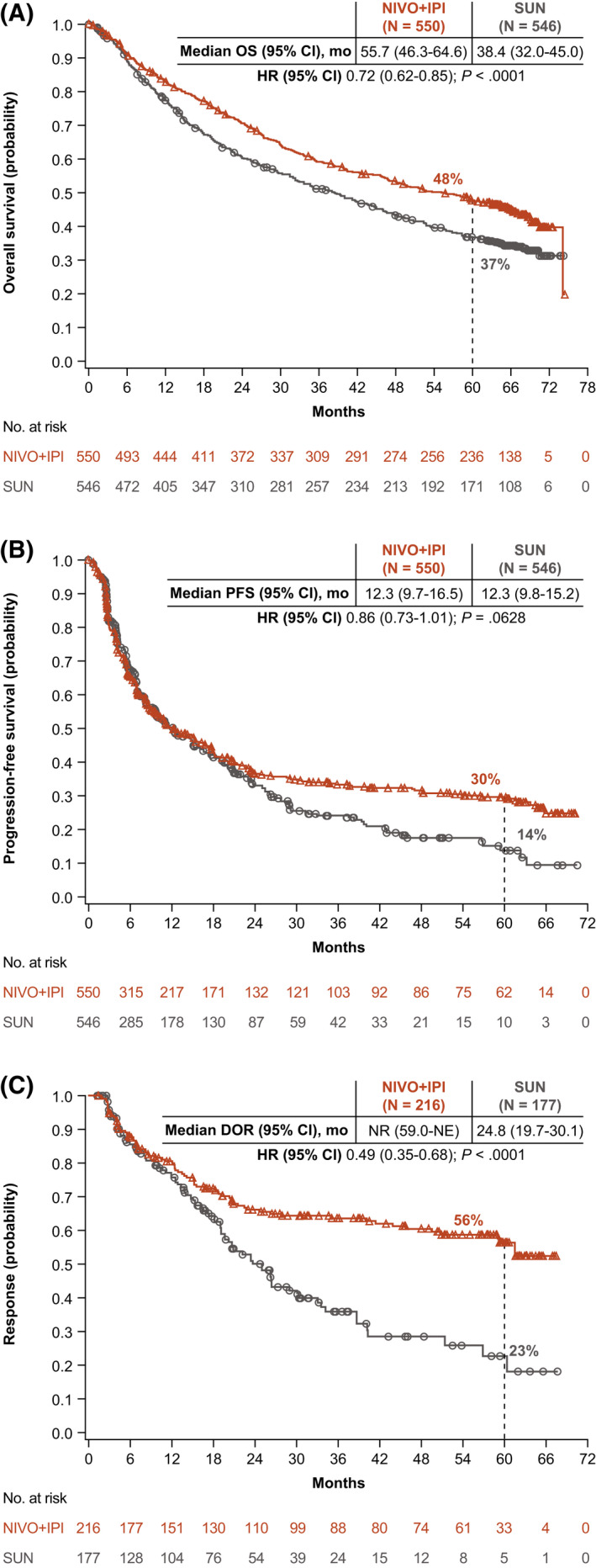
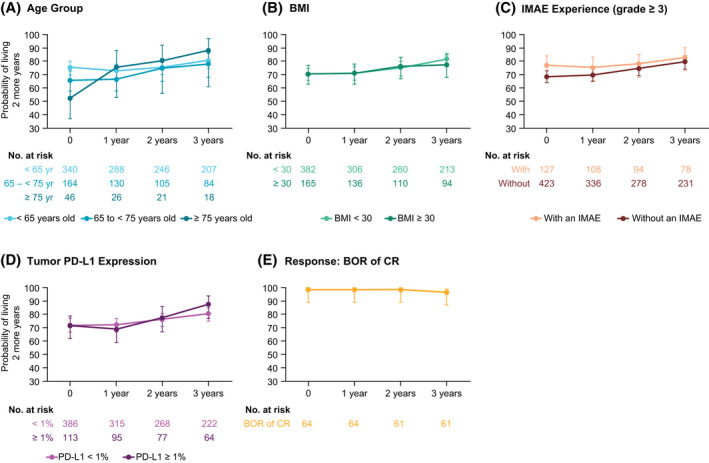
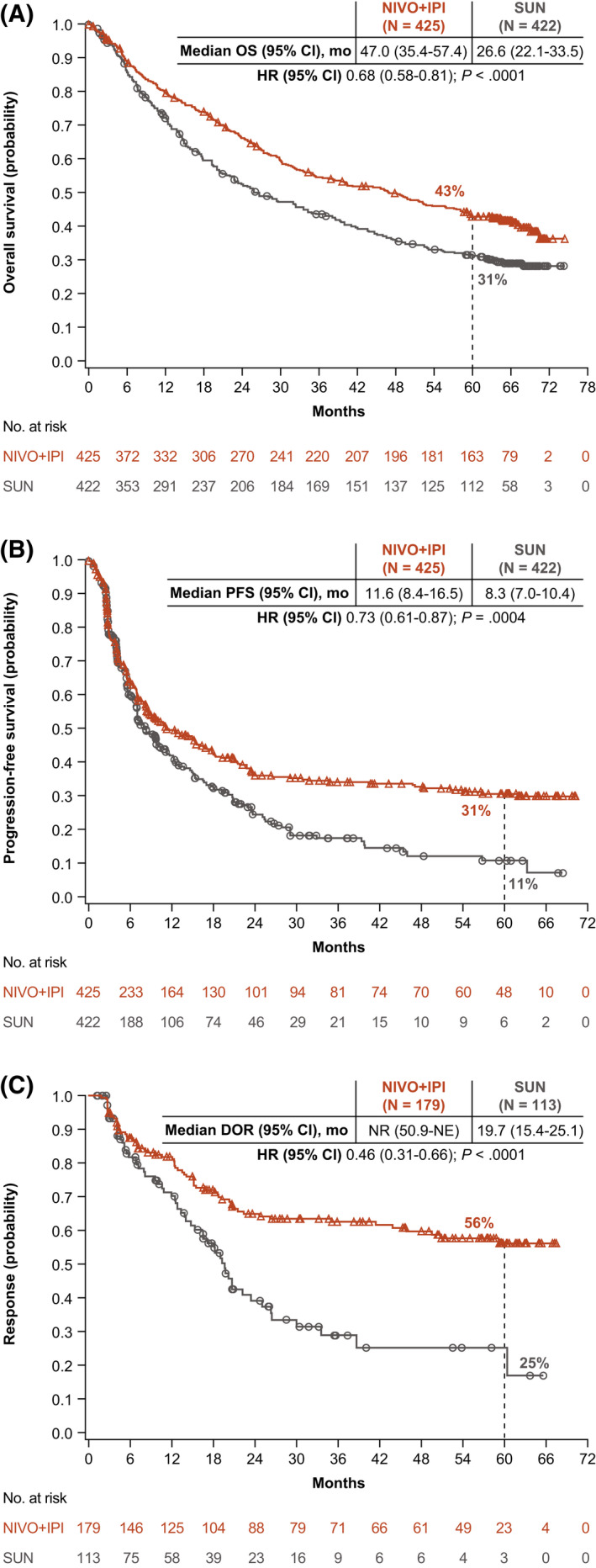
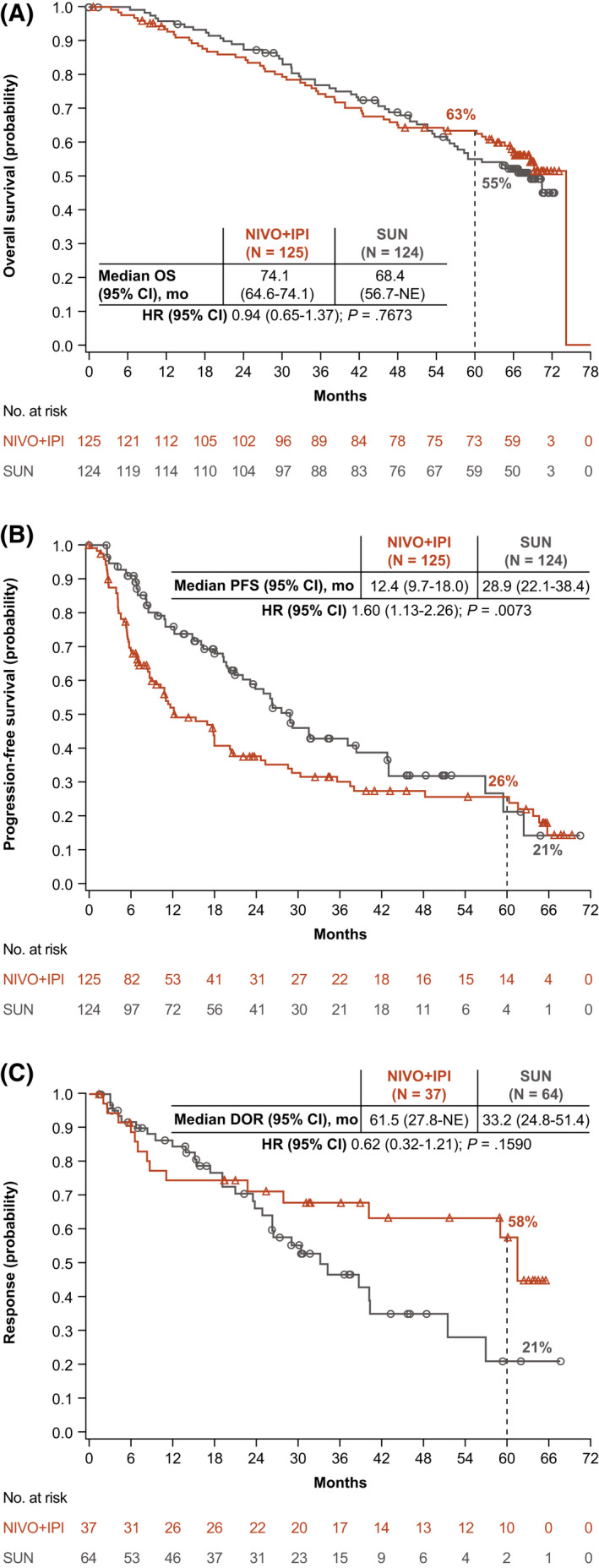
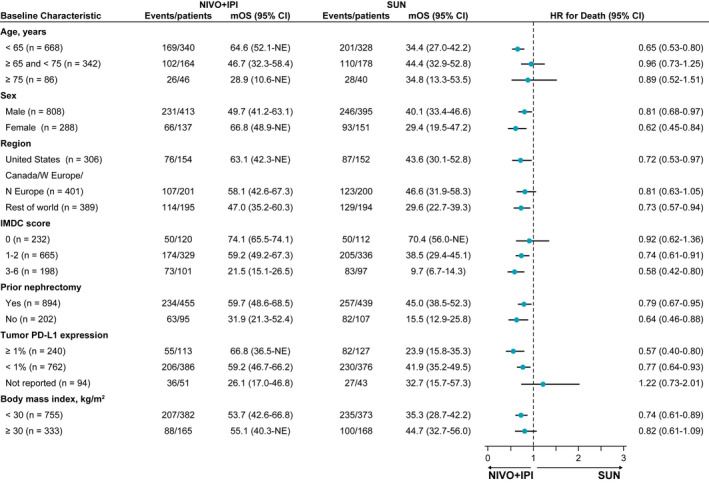
The median follow-up was 67.7 months; overall survival (median, 55.7 vs 38.4 months; hazard ratio, 0.72), progression-free survival (median, 12.3 vs 12.3 months; hazard ratio, 0.86), and objective response (39.3% vs 32.4%) benefits were maintained with NIVO+IPI versus SUN, respectively, in intent-to-treat patients (N = 550 vs 546). Point estimates for 2-year conditional overall survival beyond the 3-year landmark were higher with NIVO+IPI versus SUN (intent-to-treat patients, 81% vs 72%; intermediate-risk/poor-risk patients, 79% vs 72%; favorable-risk patients, 85% vs 72%). Conditional progression-free survival and response point estimates were also higher beyond 3 years with NIVO+IPI. Point estimates for conditional overall survival were higher or remained steady at each subsequent year of survival with NIVO+IPI in patients stratified by tumor programmed death ligand 1 expression, grade ≥3 immune-mediated adverse event experience, body mass index, and age.
Durable clinical benefits were observed with NIVO+IPI versus SUN at 5 years, the longest phase 3 follow-up for a first-line checkpoint inhibitor-based combination in patients with aRCC. Conditional estimates indicate that most patients who remained alive or in response with NIVO+IPI at 3 years remained so at 5 years.
条件生存估计为晚期肾细胞癌(aRCC)患者提供了关键的预后信息。在 CheckMate 214 中评估了疗效、安全性和条件生存结果(ClinicalTrials.gov 标识符 NCT02231749),随访时间至少为 5 年。
未经治疗的 aRCC 患者被随机分配接受nivolumab(NIVO)(3mg/kg)加 ipilimumab(IPI)(1mg/kg)每 3 周 4 个周期,然后接受 NIVO 单药或舒尼替尼(SUN)(50mg)每日(4 个 6 周周期)。疗效在意向治疗、国际转移性肾细胞癌数据库联盟中危/差危和有利风险人群中进行评估。分析了条件生存结果(在指定时间点之后 2 年仍存活、无进展或有反应的概率)。
中位随访时间为 67.7 个月;与 SUN 相比,NIVO+IPI 在意向治疗患者(N=550 对 546)中分别维持了总生存(中位,55.7 对 38.4 个月;风险比,0.72)、无进展生存(中位,12.3 对 12.3 个月;风险比,0.86)和客观反应(39.3%对 32.4%)的获益。在 3 年时间点之后,NIVO+IPI 组的 2 年条件总生存的点估计值高于 SUN 组(意向治疗患者,81%对 72%;中危/差危患者,79%对 72%;有利风险患者,85%对 72%)。NIVO+IPI 组在 3 年以上的条件无进展生存和反应的点估计值也较高。在按肿瘤程序性死亡配体 1 表达、3 级免疫介导不良事件经历、体重指数和年龄分层的患者中,NIVO+IPI 组在每个后续生存年份的条件总生存的点估计值较高或保持稳定。
在 aRCC 患者中,与 SUN 相比,NIVO+IPI 观察到了长达 5 年的持久临床获益,这是一线检查点抑制剂联合治疗最长的 3 期随访。条件估计表明,在 3 年时使用 NIVO+IPI 存活或有反应的大多数患者在 5 年时仍如此。