Sherman Jill E, Spencer John, Preisser John S, Gesler Wilbert M, Arcury Thomas A
Department of Geography, University of North Carolina, Chapel Hill, NC, USA.
Int J Health Geogr. 2005 Oct 19;4:24. doi: 10.1186/1476-072X-4-24.
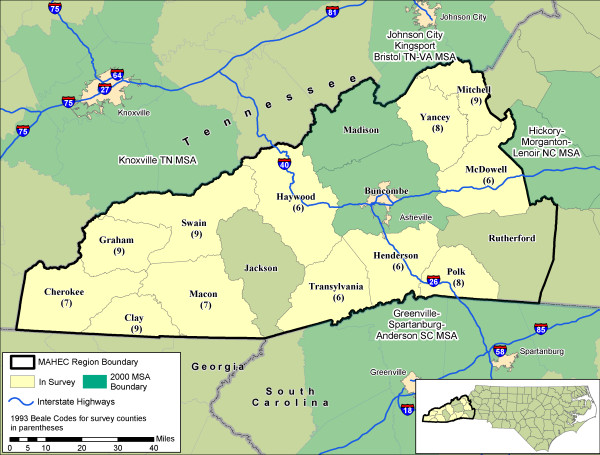
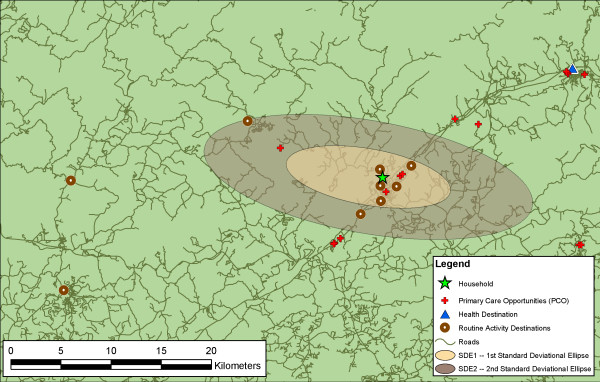
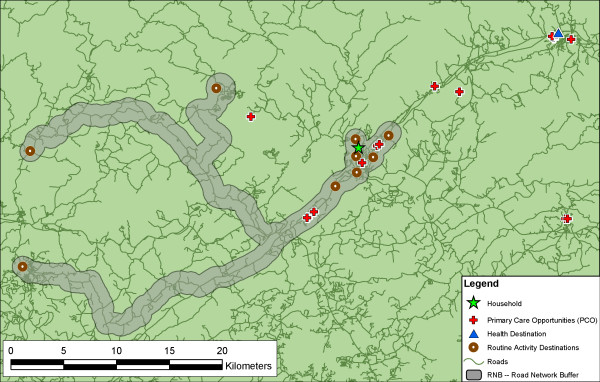
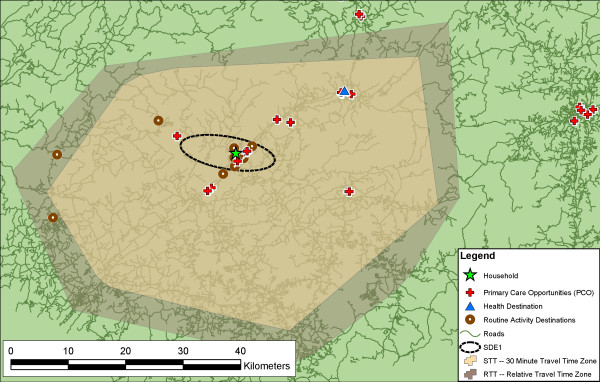
"Activity space" has been used to examine how people's habitual movements interact with their environment, and can be used to examine accessibility to healthcare opportunities. Traditionally, the standard deviational ellipse (SDE), a Euclidean measure, has been used to represent activity space. We describe the construction and application of the SDE at one and two standard deviations, and three additional network-based measures of activity space using common tools in GIS: the road network buffer (RNB), the 30-minute standard travel time polygon (STT), and the relative travel time polygon (RTT). We compare the theoretical and methodological assumptions of each measure, and evaluate the measures by examining access to primary care services, using data from western North Carolina.
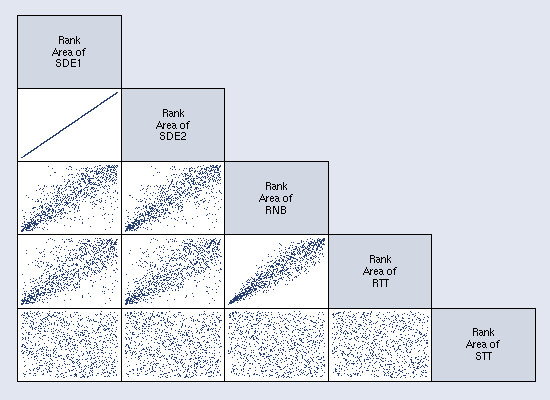
Individual accessibility is defined as the availability of healthcare opportunities within that individual's activity space. Access is influenced by the shape and area of an individual's activity space, the spatial distribution of opportunities, and by the spatial structures that constrain and direct movement through space; the shape and area of the activity space is partly a product of how it is conceptualized and measured. Network-derived measures improve upon the SDE by incorporating the spatial structures (roads) that channel movement. The area of the STT is primarily influenced by the location of a respondent's residence within the road network hierarchy, with residents living near primary roads having the largest activity spaces. The RNB was most descriptive of actual opportunities and can be used to examine bypassing. The area of the RTT had the strongest correlation with a healthcare destination being located inside the activity space.
The availability of geospatial technologies and data create multiple options for representing and operationalizing the construct of activity space. Each approach has its strengths and limitations, and presents a different view of accessibility. While the choice of method ultimately lies in the research question, interpretation of results must consider the interrelated issues of method, representation, and application. Triangulation aids this interpretation and provides a more complete and nuanced understanding of accessibility.
“活动空间”已被用于研究人们的日常活动如何与环境相互作用,并且可用于考察获得医疗保健机会的可达性。传统上,标准偏离椭圆(SDE)这一欧几里得度量方法被用于表示活动空间。我们描述了一个标准差和两个标准差下SDE的构建与应用,以及使用地理信息系统(GIS)中的常用工具对活动空间进行的另外三种基于网络的度量方法:道路网络缓冲区(RNB)、30分钟标准出行时间多边形(STT)和相对出行时间多边形(RTT)。我们比较了每种度量方法的理论和方法假设,并利用北卡罗来纳州西部的数据,通过考察初级保健服务的可及性来评估这些度量方法。
个体可及性被定义为在个体活动空间内获得医疗保健机会的情况。可及性受到个体活动空间的形状和面积、机会的空间分布以及限制和引导空间移动的空间结构的影响;活动空间的形状和面积部分取决于其概念化和测量方式。基于网络的度量方法通过纳入引导移动的空间结构(道路)对SDE进行了改进。STT的面积主要受受访者居住位置在道路网络层次结构中的影响,居住在主干道附近的居民活动空间最大。RNB最能描述实际机会,可用于考察绕行情况。RTT的面积与医疗保健目的地位于活动空间内的相关性最强。
地理空间技术和数据的可用性为表示和实施活动空间这一概念创造了多种选择。每种方法都有其优点和局限性,并呈现出不同的可及性观点。虽然方法的选择最终取决于研究问题,但结果的解释必须考虑方法、表示和应用等相互关联的问题。三角测量有助于这种解释,并能提供对可及性更完整、更细致入微的理解。