El Saghir Nagi S, Seoud Muhieddine, Khalil Mazen K, Charafeddine Maya, Salem Ziad K, Geara Fady B, Shamseddine Ali I
Department of Internal Medicine, American University of Beirut Medical Center, Beirut, Lebanon.
BMC Cancer. 2006 Jul 20;6:194. doi: 10.1186/1471-2407-6-194.
Young age remains a controversial issue as a prognostic factor in breast cancer. Debate includes patients from different parts of the world. Almost 50% of patients with breast cancer seen at the American University of Beirut Medical Center (AUBMC) are below age 50.
We reviewed 1320 patients seen at AUBMC between 1990 and 2001. We divided them in three age groups: Below 35, 35-50, and above 50. Data and survival were analyzed using Chi-square, Cox regression analysis, and Kaplan Meier.
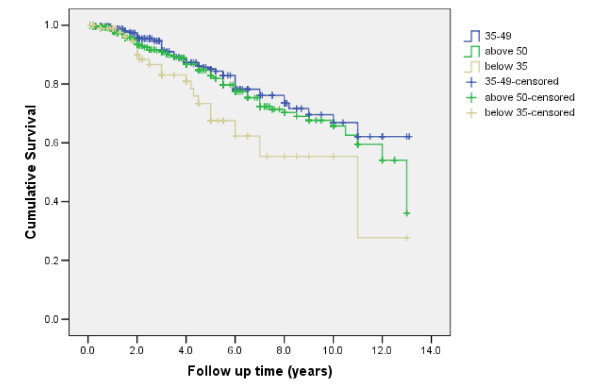
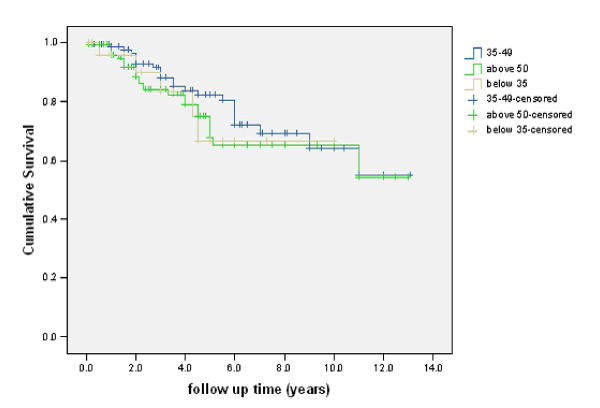
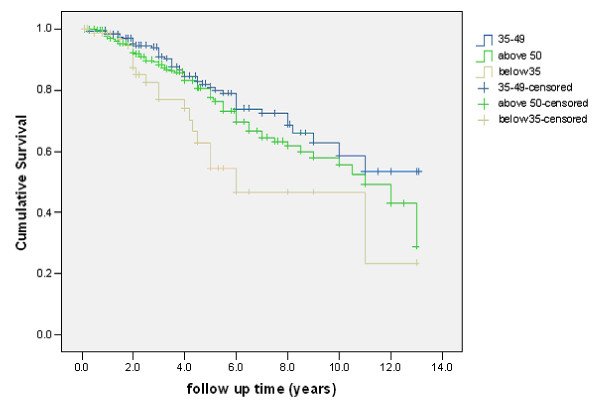
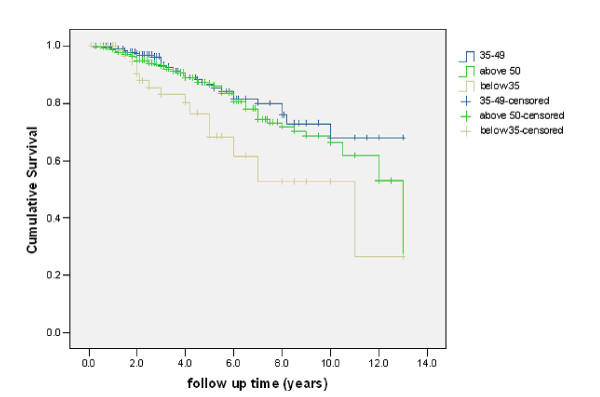
Mean age at presentation was 50.8 years. 107 patients were below age 35, 526 between 35-50 and 687 patients above age 50. Disease stages were as follows: stage I: 14.4%, stage II: 59.9%, stage III: 20% and stage IV: 5.7%. Hormone receptors were positive in 71.8% of patients below 35, in 67.6% of patients 35-50 and in 78.3% of patients above 50. Grade of tumor was higher as age at presentation was lower. More young patients received anthracycline-based adjuvant chemotherapy. Of hormone receptor-positive patients, 83.8% of those below age 35 years, 87.76% of those aged 35-50 years, and 91.2% of those aged above 50 years received adjuvant tamoxifen. The mean follow up time was 3.7 +/- 2.9 years. Time to death was the only variable analyzed for survival analysis. Excluding stage IV patients, tumor size, lymph node, tumor grade and negative hormone receptors were inversely proportional to survival. Higher percentage of young patients at presentation developed metastasis (32.4% of patients below 35, as compared to 22.9% of patients 35-50 and 22.8% of patients above 50) and had a worse survival. Young age had a negative impact on survival of patients with positive axillary lymph nodes, and survival of patients with positive hormonal receptors, but not on survival of patients with negative lymph nodes, or patients with negative hormonal receptors.
Young age at presentation conferred a worse prognosis in spite of a higher than expected positive hormone receptor status, more anthracycline-based adjuvant chemotherapy and equivalent adjuvant tamoxifen hormonal therapy in younger patients. This negative impact on survival was seen in patients with positive lymph nodes and those with positive hormonal receptors.
年轻作为乳腺癌的一个预后因素,仍然是一个有争议的问题。争论涉及来自世界不同地区的患者。在美国贝鲁特美国大学医学中心(AUBMC)就诊的乳腺癌患者中,近50%年龄在50岁以下。
我们回顾了1990年至2001年间在AUBMC就诊的1320例患者。我们将他们分为三个年龄组:35岁以下、35 - 50岁和50岁以上。使用卡方检验、Cox回归分析和Kaplan Meier法分析数据和生存率。
就诊时的平均年龄为50.8岁。107例患者年龄在35岁以下,526例在35 - 50岁之间,687例患者年龄在50岁以上。疾病分期如下:I期:14.4%,II期:59.9%,III期:20%,IV期:5.7%。35岁以下患者中71.8%激素受体阳性,35 - 50岁患者中67.6%阳性,50岁以上患者中78.3%阳性。肿瘤分级随着就诊年龄降低而更高。更多年轻患者接受了以蒽环类为基础的辅助化疗。在激素受体阳性的患者中,35岁以下患者中有83.8%、35 - 50岁患者中有87.7%、50岁以上患者中有91.2%接受了辅助他莫昔芬治疗。平均随访时间为3.7±2.九年。生存分析仅分析死亡时间这一变量。排除IV期患者后,肿瘤大小淋巴结、肿瘤分级和激素受体阴性与生存率呈负相关。就诊时年轻患者发生转移的比例更高(35岁以下患者中有32.4%发生转移,相比之下~ 35 - 50岁患者中有22.9%,50岁以上患者中有22.8%),且生存率更差。年轻对腋窝淋巴结阳性患者以及激素受体阳性患者的生存有负面影响,但对淋巴结阴性患者或激素受体阴性患者的生存没有影响。
尽管年轻患者激素受体阳性率高于预期、接受了更多以蒽环类为基础的辅助化疗以及等效的辅助他莫昔芬激素治疗,但就诊时年轻仍预示着更差的预后。这种对生存的负面影响在淋巴结阳性患者和激素受体阳性患者中可见。