Tollefsen S E, Heath-Monnig E, Cascieri M A, Bayne M L, Daughaday W H
Edward Mallinckrodt Department of Pediatrics, Washington University School of Medicine, St.Louis, Missouri 63110.
J Clin Invest. 1991 Apr;87(4):1241-50. doi: 10.1172/JCI115125.
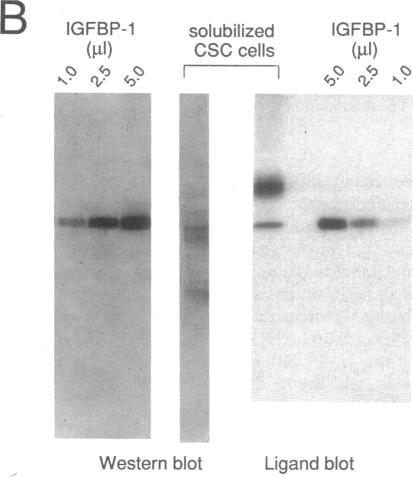
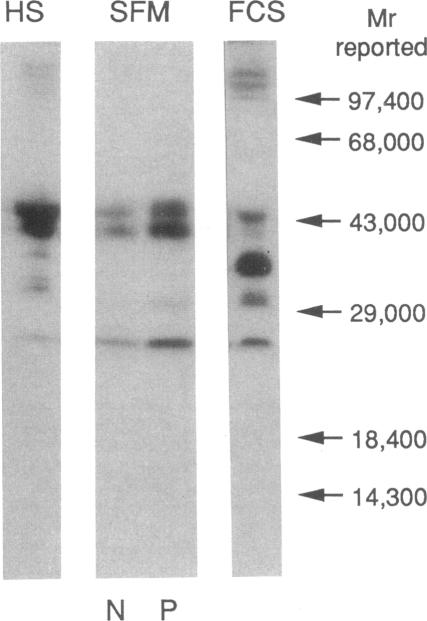
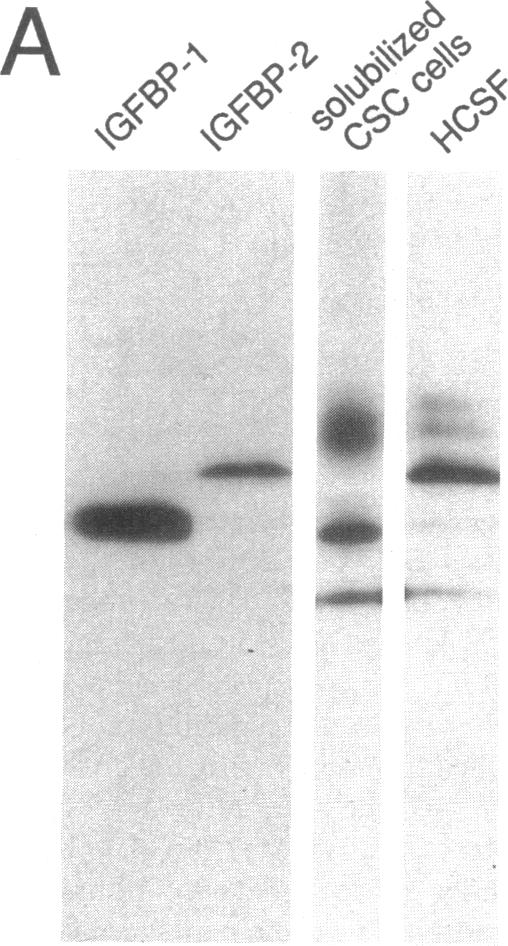
The ED50 of insulin-like growth factor (IGF)-I-stimulated alpha-aminoisobutyric acid (AIB) uptake (mean +/- SD) in cultured fibroblasts from a child with short stature that we have reported (1.40 +/- 0.24 nM), is significantly higher than the ED50 of IGF-I-stimulated AIB uptake in fibroblasts from 11 normal subjects (0.42 +/- 0.12 nM) and from 127 short children (0.35 +/- 0.11 nM). Similarly, the ED50 of IGF-I-stimulated thymidine incorporation in fibroblasts from this child is 2.8 times higher than that in fibroblasts from four normal subjects. To minimize potential modulation of IGF-I action by endogenous IGF binding proteins in these assays, fibroblast responsiveness to [Q3,A4,Y15,L16]IGF-I, an IGF-I variant that has a 600-fold reduced affinity for serum IGF binding proteins, has been examined. The biological activity of this variant is comparable in the patient's and normal fibroblasts, suggesting that the resistance to IGF-I action cannot be attributed to a defective IGF-I receptor. To investigate directly the possibility that IGF-I sensitivity in the patient's fibroblasts is reduced by endogenous IGF binding proteins (IGFBP), binding proteins that are secreted into AIB assay buffer during a 3-h collection and that are cell-associated at the end of the collection have been analyzed. Ligand blot analysis of conditioned AIB assay buffer demonstrates that fibroblasts from the patient secrete 1.3-2.2 times more of Mr 46,400/42,900, 32,000, and 26,800 binding proteins than normal fibroblasts. The major difference between fibroblasts from the patient and from normal subjects is a striking 10-fold increase in the amount of a cell surface Mr 32,000 binding protein in the patient's fibroblasts. The Mr 32,000 binding protein is similar in size to IGFB-1 and different from IGFBP-2 and IGFBP-3, but it does not cross-react with an antibody against IGFBP-1. We conclude that the resistance to IGF-I action in the patient's fibroblasts is caused by an abnormal production and/or cell association of IGF binding proteins.
我们曾报道过一名身材矮小儿童,其培养的成纤维细胞中胰岛素样生长因子(IGF)-I刺激的α-氨基异丁酸(AIB)摄取的半数有效剂量(ED50,均值±标准差)为(1.40±0.24 nM),显著高于11名正常受试者(0.42±0.12 nM)及127名身材矮小儿童(0.35±0.11 nM)的成纤维细胞中IGF-I刺激的AIB摄取的ED50。同样,该儿童成纤维细胞中IGF-I刺激的胸苷掺入的ED50比4名正常受试者的成纤维细胞中的高2.8倍。为了在这些检测中尽量减少内源性IGF结合蛋白对IGF-I作用的潜在调节,已检测了成纤维细胞对[Q3,A4,Y15,L16]IGF-I(一种对血清IGF结合蛋白亲和力降低600倍的IGF-I变体)的反应性。该变体在患者和成纤维细胞中的生物活性相当,这表明对IGF-I作用的抵抗不能归因于IGF-I受体缺陷。为了直接研究患者成纤维细胞中IGF-I敏感性降低是否由内源性IGF结合蛋白(IGFBP)引起,已分析了在3小时收集过程中分泌到AIB检测缓冲液中且在收集结束时与细胞相关的结合蛋白。对条件性AIB检测缓冲液的配体印迹分析表明,患者的成纤维细胞分泌的分子量为46,400/42,900、32,000和26,800的结合蛋白比正常成纤维细胞多1.3 - 2.2倍。患者和成纤维细胞之间的主要差异在于患者成纤维细胞中一种细胞表面分子量为32,000的结合蛋白的量显著增加了10倍。分子量为32,