Rizoli Sandro B, Boffard Kenneth D, Riou Bruno, Warren Brian, Iau Philip, Kluger Yoram, Rossaint Rolf, Tillinger Michael
Department of Surgery and Critical Care Medicine, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, M4N 3M5 Canada.
Crit Care. 2006;10(6):R178. doi: 10.1186/cc5133.
We conducted a post-hoc analysis on the effect of recombinant factor VIIa (rFVIIa) on coagulopathic patients from two randomized, placebo-controlled, double-blind trials of rFVIIa as an adjunctive therapy for bleeding in patients with severe trauma.
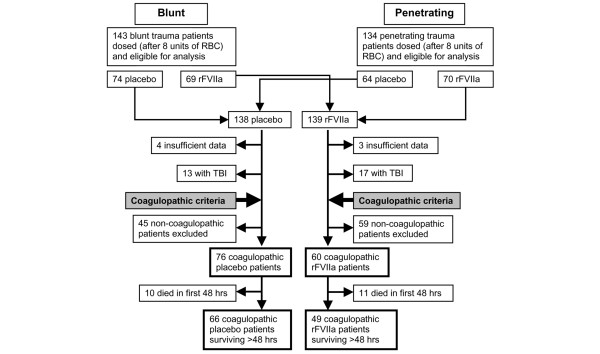
Blunt and penetrating trauma patients were randomly assigned to rFVIIa (200 + 100 + 100 microg/kg) at 0, 1, and 3 hours after transfusion of 8 units of red blood cells (RBCs) or to placebo. Subjects were monitored for 48 hours post-dosing and followed for 30 days. Coagulopathy was retrospectively defined as transfusion of fresh frozen plasma (FFP) (>1 unit of FFP per 4 units of RBCs), FFP in addition to whole blood, and transfusion of platelets and/or cryoprecipitate.
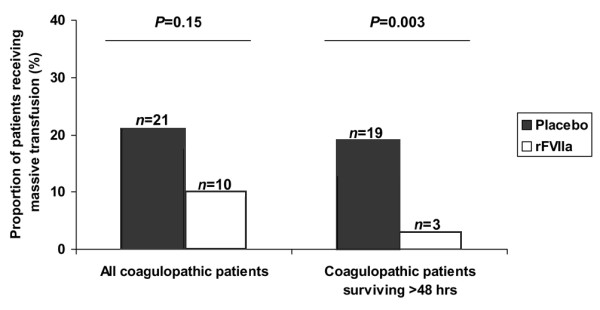
Sixty rFVIIa-treated and 76 placebo subjects were retrospectively identified as being coagulopathic. No significant differences were noted in baseline characteristics. The rFVIIa-treated coagulopathic subgroup consumed significantly less blood product: RBC transfusion decreased by 2.6 units for the whole study population (P = 0.02) and by 3.5 units among patients surviving more than 48 hours (P < 0.001). Transfusion of FFP (1,400 versus 660 ml, P < 0.01), platelet (300 versus 100 ml, P = 0.01), and massive transfusions (29% versus 6%, P < 0.01) also dropped significantly. rFVIIa reduced multi-organ failure and/or acute respiratory distress syndrome in the coagulopathic patients (3% versus 20%, P = 0.004), whereas thromboembolic events were equally present in both groups (3% versus 4%, P = 1.00).
Coagulopathic trauma patients appear to derive particular benefit from early adjunctive rFVIIa therapy.
我们对重组凝血因子VIIa(rFVIIa)在两项随机、安慰剂对照、双盲试验中对凝血病患者的疗效进行了事后分析,这两项试验将rFVIIa作为严重创伤患者出血的辅助治疗方法。
钝性和穿透性创伤患者在输注8单位红细胞(RBC)后0、1和3小时被随机分配接受rFVIIa(200 + 100 + 100微克/千克)或安慰剂。给药后对受试者监测48小时,并随访30天。凝血病被回顾性定义为输注新鲜冰冻血浆(FFP)(每4单位RBC输注>1单位FFP)、除全血外还输注FFP以及输注血小板和/或冷沉淀。
回顾性确定60例接受rFVIIa治疗和76例安慰剂受试者患有凝血病。基线特征方面未观察到显著差异。接受rFVIIa治疗的凝血病亚组消耗的血液制品显著减少:整个研究人群的RBC输注减少2.6单位(P = 0.02),存活超过48小时的患者中减少3.5单位(P < 0.001)。FFP输注量(1400对660毫升,P < 0.01)、血小板输注量(300对100毫升,P = 0.01)和大量输血(29%对6%,P < 0.01)也显著下降。rFVIIa降低了凝血病患者的多器官功能衰竭和/或急性呼吸窘迫综合征发生率(3%对20%,P = 0.004),而两组血栓栓塞事件发生率相当(3%对4%,P = 1.00)。
凝血病创伤患者似乎从早期辅助rFVIIa治疗中特别受益。