Gerstl Sibylle, Cohuet Sandra, Edoh Kodjo, Brasher Christopher, Lesage Alexandre, Guthmann Jean-Paul, Checchi Francesco
Epicentre, Paris, France.
Malar J. 2007 Jul 18;6:94. doi: 10.1186/1475-2875-6-94.
In 2003, artesunate-amodiaquine (AS+AQ) was introduced as the new first-line treatment for uncomplicated malaria in Burundi. After confirmed diagnosis, treatment was delivered at subsidized prices in public health centres. Nine months after its implementation a study was carried out to assess whether children below five years of age with uncomplicated malaria were actually receiving AS+AQ.
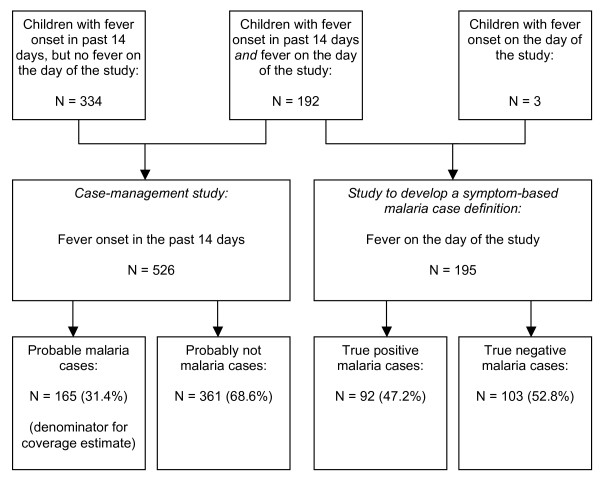
A community-based study was conducted in Makamba province. Randomly selected households containing one or more children under five with reported fever onset within fourteen days before the study date were eligible. Case-management information was collected based on caregiver recall. A case definition of symptomatic malaria from observations of children presenting a confirmed malaria episode on the day of the survey was developed. Based on this definition, those children who had probable malaria among those with fever onset in the 14 days prior to the study were identified retrospectively. Treatment coverage with AS+AQ was then estimated among these probable malaria cases.
Out of 195 children with fever on the day of the study, 92 were confirmed as true malaria cases and 103 tested negative. The combination of 'loss of appetite', 'sweating', 'shivering' and 'intermittent fever' yielded the highest possible positive predictive value, and was chosen as the case definition of malaria. Out of 526 children who had had fever 14 days prior to the survey, 165 (31.4%) were defined as probable malaria cases using this definition. Among them, 20 (14.1%) had been treated with AS+AQ, 10 with quinine (5%), 68 (41%) received non-malaria treatments, and 67 got traditional treatment or nothing (39.9%). Most people sought treatment from public health centres (23/99) followed by private clinics (15/99, 14.1%). The median price paid for AS+AQ was 0.5 US$.
AS+AQ was the most common treatment for patients with probable malaria at public health centres, but coverage was low due to low health centre utilisation and apparently inappropriate prescribing. In addition, AS+AQ was given to patients at a price ten times higher than the subsidized price. The availability and proper use of ACTs should be monitored and maximized after their introduction in order to have a significant impact on the burden of malaria.
2003年,青蒿琥酯-阿莫地喹(AS+AQ)被引入布隆迪作为单纯性疟疾的新一线治疗药物。确诊后,在公共卫生中心以补贴价格提供治疗。实施九个月后,开展了一项研究以评估五岁以下单纯性疟疾患儿是否实际接受了AS+AQ治疗。
在马坎巴省开展了一项基于社区的研究。随机选择的家庭中若有一名或多名五岁以下儿童,且在研究日期前十四天内有发热症状,则该家庭符合条件。根据照顾者的回忆收集病例管理信息。根据调查当天确诊疟疾发作儿童的观察结果制定了有症状疟疾的病例定义。基于此定义,回顾性确定在研究前14天内发热儿童中可能患有疟疾的儿童。然后在这些可能患有疟疾的病例中估计AS+AQ的治疗覆盖率。
在研究当天发热的195名儿童中,92名被确诊为真正的疟疾病例,103名检测呈阴性。“食欲不振”、“出汗”、“颤抖”和“间歇性发热”的组合产生了最高的阳性预测值,并被选为疟疾的病例定义。在调查前14天内发热的526名儿童中,165名(31.4%)根据此定义被确定为可能的疟疾病例。其中,20名(14.1%)接受了AS+AQ治疗,10名接受了奎宁治疗(5%),68名(41%)接受了非疟疾治疗,67名接受了传统治疗或未接受任何治疗(39.9%)。大多数人在公共卫生中心寻求治疗(23/99),其次是私人诊所(15/99,14.1%)。AS+AQ的支付中位数价格为0.5美元。
AS+AQ是公共卫生中心可能患有疟疾患者最常用的治疗药物,但由于卫生中心利用率低和明显不适当的处方,覆盖率较低。此外,AS+AQ以比补贴价格高十倍的价格提供给患者。在引入青蒿素联合疗法后,应监测并最大限度地提高其可及性和合理使用,以便对疟疾负担产生重大影响。