Makris Demosthenes, Scherpereel Arnaud, Copin Marie Christine, Colin Guillaume, Brun Luc, Lafitte Jean Jacques, Marquette Charles Hugo
Pulmonary and Thoracic Oncology Department, CHRU of Lille, Lille, France.
BMC Cancer. 2007 Aug 5;7:150. doi: 10.1186/1471-2407-7-150.
Erlotinib is a Human Epidermal Growth Factor Receptor Type 1/tyrosine kinase (EGFR) inhibitor which is used for non-small-cell lung cancer treatment. Despite that erlotinib is considered to have a favorable safety profile, adverse events such as interstitial lung disease (ILD) were reported in pivotal studies. The authors report the first histologically confirmed case of fatal ILD associated with erlotinib therapy.
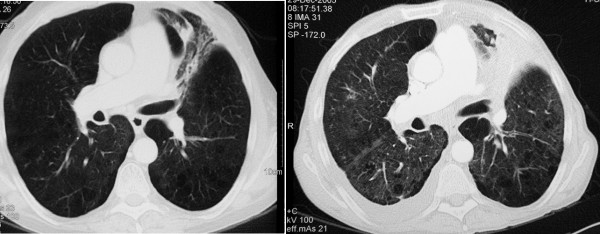
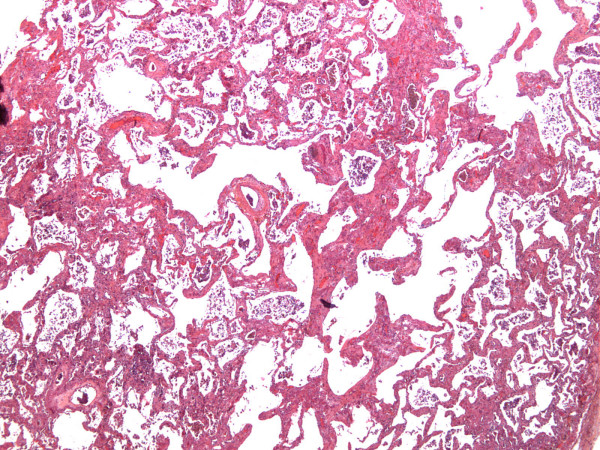
The medical record of a patient who developed fatal ILD after receiving erlotinib treatment was reviewed to identify the cause of death and other factors potentially contributive to this adverse outcome. A 55-year-old smoker with no evidence of pre-existing interstitial disease developed bilateral ILD and respiratory failure which could be explained only as a toxicity of erlotinib. He had a history of stage IV left upper lobe squamous-cell carcinoma for which he had received three successive regimens of chemotherapy (ifosfamide plus gemcitabine, docetaxel, mitomycin plus navelbine), followed five months later by erlotinib. At initiation of erlotinib treatment there were no radiological signs suggestive of ILD disease or apparent clinical signs of respiratory distress. While the patient completed two months with erlotinib therapy he developed bilateral interstitial infiltrates; despite discontinuation of erlotinib he was admitted with respiratory failure two weeks later. Diagnostic work up for other causes of pneumonitis including infectious diseases, congestive cardiac failure and pulmonary infraction was negative. Empiric treatment with oxygene, corticosteroids and later with cyclophosphamide was ineffective and the patient progressively deteriorated and died. The clinical and post-mortem examination findings are presented and the possible association relationship between erlotinib induced ILD and previous chemotherapy is discussed.
Physicians should be alert to the fact that erlotinib related ILD, although infrequent, is potential fatal. The association between selective EGFR-inhibitors and ILD should be further investigated.
厄洛替尼是一种人表皮生长因子受体1/酪氨酸激酶(EGFR)抑制剂,用于治疗非小细胞肺癌。尽管厄洛替尼被认为具有良好的安全性,但在关键研究中报告了诸如间质性肺病(ILD)等不良事件。作者报告了首例经组织学证实的与厄洛替尼治疗相关的致命性ILD病例。
回顾了一名接受厄洛替尼治疗后发生致命性ILD患者的病历,以确定死亡原因及其他可能导致这一不良后果的因素。一名55岁吸烟者,无既往间质性疾病证据,出现双侧ILD和呼吸衰竭,这只能解释为厄洛替尼的毒性作用。他有IV期左上叶鳞状细胞癌病史,曾接受过三个连续化疗方案(异环磷酰胺加吉西他滨、多西他赛、丝裂霉素加长春瑞滨),五个月后接受厄洛替尼治疗。在开始厄洛替尼治疗时,没有提示ILD疾病的放射学征象或明显的呼吸窘迫临床体征。在患者接受厄洛替尼治疗两个月时,出现双侧间质性浸润;尽管停用了厄洛替尼,但两周后他因呼吸衰竭入院。对包括感染性疾病、充血性心力衰竭和肺梗死在内的其他肺炎病因的诊断性检查均为阴性。给予氧气、皮质类固醇以及后来的环磷酰胺进行经验性治疗均无效,患者病情逐渐恶化并死亡。本文展示了临床和尸检结果,并讨论了厄洛替尼诱导的ILD与先前化疗之间可能的关联关系。
医生应警惕,厄洛替尼相关的ILD虽然不常见,但有潜在致命性。选择性EGFR抑制剂与ILD之间的关联应进一步研究。