van der Vorst Maria M J, den Hartigh Jan, Wildschut Enno, Tibboel Dick, Burggraaf Jacobus
Centre for Human Drug Research, Leiden, The Netherlands.
Crit Care. 2007;11(5):R111. doi: 10.1186/cc6146.
The objective of the present study was to explore a continuous intravenous furosemide regimen that adapts to urine output in neonates treated with extracorporeal membrane oxygenation (ECMO).
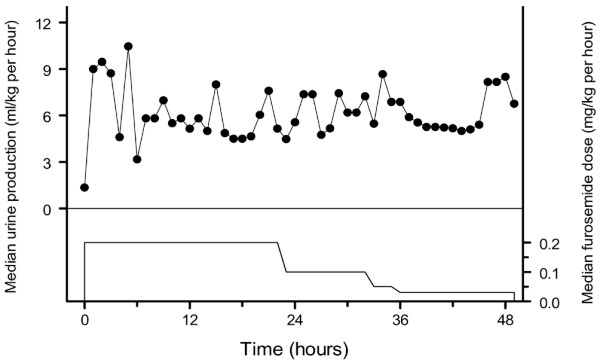
Seven neonates admitted to a paediatric surgical intensive care unit for ECMO therapy were treated with a furosemide regimen consisting of a loading bolus (1-2 mg/kg) followed by a continuous infusion at 0.2 mg/kg per hour, which was adjusted according to the target urine production of 6 ml/kg per hour. Therapeutic drug monitoring for furosemide concentrations in blood was performed.
The mean +/- standard deviation furosemide dose was 0.17 +/- 0.06 mg/kg per hour, 0.08 +/- 0.04 mg/kg per hour and 0.12 +/- 0.07 mg/kg per hour, respectively, on the first day, second day and third day of the study. The median (range of the urine production of the study subjects) urine production over the consecutive study days was 6.8 (0.8-8.4) mg/kg per hour, 6.0 (4.7-8.9) mg/kg per hour and 5.4 (3.4-10.1) ml/kg per hour. The target urine production was reached after a median time of 7 (3-37) hours. The regimen was haemodynamically well tolerated and the median furosemide serum concentration was 3.1 (0.4-12.9) mug/ml, well below the toxic level.
The evaluated furosemide infusion appears an effective means to reduce volume overload in neonates treated with ECMO. The data of this preliminary study suggest that the starting dose of furosemide was too high, however, because the urine output was excessive and required frequent adaptations. The results of this study therefore indicate that a novel pharmacokinetic/pharmacodynamic model needs to be developed for neonates treated with ECMO.
本研究的目的是探索一种适用于接受体外膜肺氧合(ECMO)治疗的新生儿尿量的持续静脉注射速尿方案。
七名入住儿科外科重症监护病房接受ECMO治疗的新生儿采用速尿方案治疗,先给予负荷剂量(1 - 2毫克/千克),然后以每小时0.2毫克/千克的速度持续输注,并根据每小时6毫升/千克的目标尿量进行调整。对血液中的速尿浓度进行治疗药物监测。
在研究的第一天、第二天和第三天,速尿的平均±标准差剂量分别为每小时0.17±0.06毫克/千克、每小时0.08±0.04毫克/千克和每小时0.12±0.07毫克/千克。在连续的研究日中,研究对象的中位数(尿量范围)尿量分别为每小时6.8(0.8 - 8.4)毫克/千克、每小时6.0(4.7 - 8.9)毫克/千克和每小时5.4(3.4 - 10.1)毫升/千克。达到目标尿量的中位时间为7(3 - 37)小时。该方案在血流动力学上耐受性良好,速尿血清浓度中位数为3.1(0.4 - 12.9)微克/毫升,远低于中毒水平。
所评估的速尿输注似乎是减少接受ECMO治疗的新生儿容量超负荷的有效手段。然而,这项初步研究的数据表明,速尿的起始剂量过高,因为尿量过多且需要频繁调整。因此,本研究结果表明,需要为接受ECMO治疗的新生儿开发一种新的药代动力学/药效学模型。