Taranova Anna G, Maldonado David, Vachon Celine M, Jacobsen Elizabeth A, Abdala-Valencia Hiam, McGarry Michael P, Ochkur Sergei I, Protheroe Cheryl A, Doyle Alfred, Grant Clive S, Cook-Mills Joan, Birnbaumer Lutz, Lee Nancy A, Lee James J
Department of Biochemistry and Molecular Biology, Divisions of Pulmonary Medicine, Mayo Clinic Arizona, Scottsdale, Arizona 85259, USA.
Cancer Res. 2008 Oct 15;68(20):8582-9. doi: 10.1158/0008-5472.CAN-08-1673.
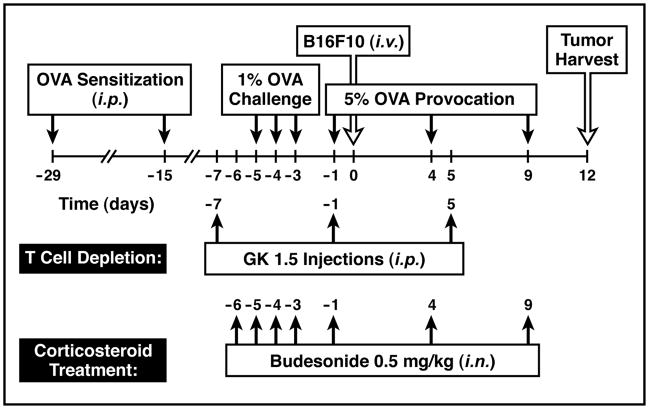
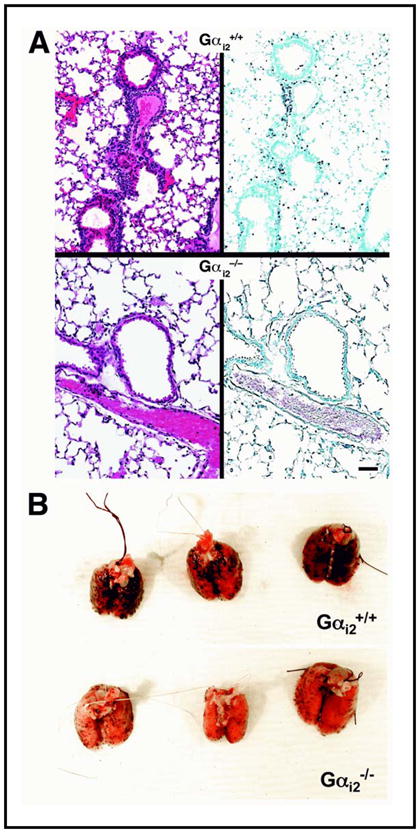
Allergen-induced respiratory inflammation facilitates and/or elicits the extravasation of proinflammatory leukocytes by well-understood mechanisms that mediate the movement of multiple cell types. The nonspecific character of these pathways led us to hypothesize that circulating cancer cells use similar mechanisms, promoting secondary tumor formation at distal sites. To test this hypothesis, the frequency of metastasis to the lung as a function of allergic pulmonary inflammation was assessed following the i.v. injection of B16-F10 melanoma cells in mice. These studies showed that allergen-induced pulmonary inflammation resulted in a >3-fold increase in lung metastases. This increase was dependent on CD4(+) T-cell activities; however, it occurred independent of the induced eosinophilia associated with allergen provocation. Interventional strategies showed that existing therapeutic modalities for asthma, such as inhaled corticosteroids, were sufficient to block the enhanced pulmonary recruitment of cancer cells from circulation. Additional mechanistic studies further suggested that the ability of circulating cancer cells to extravasate to surrounding lung tissues was linked to the activation of the vascular endothelium via one or more Galpha(i)-coupled receptors. Interestingly, a survey of a clinical breast cancer surgical database showed that the incidence of asthma was higher among patients with lung metastases. Thus, our data show that allergic respiratory inflammation may represent a risk factor for the development of lung metastases and suggest that amelioration of the pulmonary inflammation associated with asthma will have a direct and immediate benefit to the 7% to 8% of breast cancer patients with this lung disease.
变应原诱导的呼吸道炎症通过介导多种细胞类型移动的已知机制促进和/或引发促炎白细胞的渗出。这些途径的非特异性使我们推测循环癌细胞利用类似机制,促进远端部位继发性肿瘤的形成。为了验证这一假设,在给小鼠静脉注射B16-F10黑色素瘤细胞后,评估了肺转移频率与变应性肺部炎症的关系。这些研究表明,变应原诱导的肺部炎症导致肺转移增加了3倍以上。这种增加依赖于CD4(+) T细胞活性;然而,它的发生与变应原激发相关的诱导嗜酸性粒细胞增多无关。干预策略表明,现有的哮喘治疗方法,如吸入皮质类固醇,足以阻止循环中癌细胞向肺部的增强募集。进一步的机制研究表明,循环癌细胞向周围肺组织渗出的能力与通过一种或多种Gα(i)偶联受体激活血管内皮有关。有趣的是,对一个临床乳腺癌手术数据库的调查显示,肺转移患者中哮喘的发病率更高。因此,我们的数据表明,变应性呼吸道炎症可能是肺转移发生的一个危险因素,并表明改善与哮喘相关的肺部炎症将对7%至8%患有这种肺部疾病的乳腺癌患者有直接和即时的益处。