National Centre for Epidemiology and Population Health, The Australian National University, Acton, Australia.
PLoS Med. 2009 Nov;6(11):e1000181. doi: 10.1371/journal.pmed.1000181. Epub 2009 Nov 10.
Bone mineral density is known to decrease rapidly after the menopause. There is limited evidence about the separate contributions of a woman's age, menopausal status and age at menopause to the incidence of hip fracture.
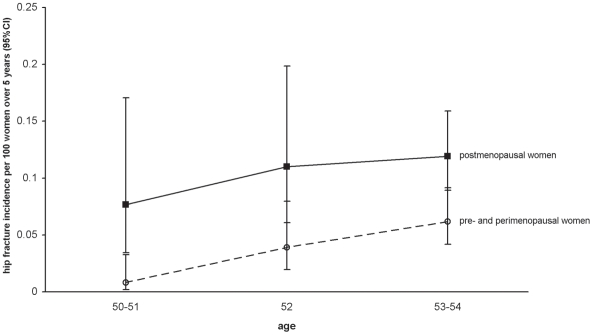
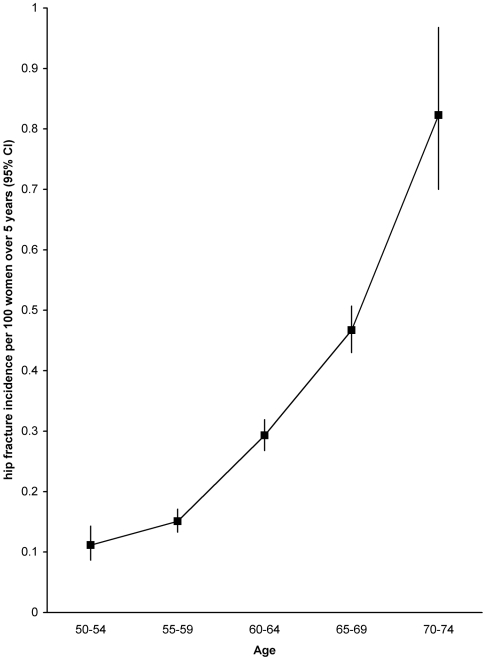
Over one million middle-aged women joined the UK Million Women Study in 1996-2001 providing information on their menopausal status, age at menopause, and other factors, which was updated, where possible, 3 y later. All women were registered with the UK National Health Service (NHS) and were routinely linked to information on cause-specific admissions to NHS hospitals. 561,609 women who had never used hormone replacement therapy and who provided complete information on menopausal variables (at baseline 25% were pre/perimenopausal and 75% postmenopausal) were followed up for a total of 3.4 million woman-years (an average 6.2 y per woman). During follow-up 1,676 (0.3%) were admitted to hospital with a first incident hip fracture. Among women aged 50-54 y the relative risk (RR) of hip fracture risk was significantly higher in postmenopausal than premenopausal women (adjusted RR 2.22, 95% confidence interval [CI] 1.22-4.04; p = 0.009); there were too few premenopausal women aged 55 y and over for valid comparisons. Among postmenopausal women, hip fracture incidence increased steeply with age (p<0.001), with rates being about seven times higher at age 70-74 y than at 50-54 y (incidence rates of 0.82 versus 0.11 per 100 women over 5 y). Among postmenopausal women of a given age there was no significant difference in hip fracture incidence between women whose menopause was due to bilateral oophorectomy compared to a natural menopause (adjusted RR 1.20, 95% CI 0.94-1.55; p = 0.15), and age at menopause had little, if any, effect on hip fracture incidence.
At around the time of the menopause, hip fracture incidence is about twice as high in postmenopausal than in premenopausal women, but this effect is short lived. Among postmenopausal women, age is by far the main determinant of hip fracture incidence and, for women of a given age, their age at menopause has, at most, a weak additional effect. Please see later in the article for the Editors' Summary.
众所周知,女性绝经后骨密度会迅速下降。关于女性年龄、绝经状态和绝经年龄对髋部骨折发生率的单独影响,证据有限。
1996 年至 2001 年期间,超过 100 万名中年女性参加了英国百万女性研究,提供了她们的绝经状态、绝经年龄和其他因素的信息,在可能的情况下,3 年后进行了更新。所有女性都在英国国家医疗服务体系(NHS)注册,并定期与 NHS 医院特定病因入院信息相关联。561609 名从未使用过激素替代疗法且提供完整绝经变量信息的女性(基线时 25%处于围绝经期和 75%处于绝经后)共随访了 340 万妇女年(平均每位女性随访 6.2 年)。随访期间,有 1676 名(0.3%)女性首次因髋部骨折住院。在 50-54 岁的女性中,绝经后女性髋部骨折风险的相对风险(RR)明显高于围绝经期女性(调整 RR 2.22,95%置信区间[CI] 1.22-4.04;p=0.009);55 岁及以上的围绝经期女性人数太少,无法进行有效比较。在绝经后女性中,髋部骨折发生率随年龄急剧上升(p<0.001),70-74 岁时的发生率约为 50-54 岁时的 7 倍(5 年期间的发生率分别为每 100 名女性 0.82 和 0.11)。在给定年龄的绝经后女性中,由于双侧卵巢切除术导致的绝经与自然绝经的髋部骨折发生率无显著差异(调整 RR 1.20,95%CI 0.94-1.55;p=0.15),绝经年龄对髋部骨折发生率影响很小,如果有影响的话。
在绝经前后,绝经后女性髋部骨折的发生率大约是绝经前女性的两倍,但这种影响是短暂的。在绝经后女性中,年龄是髋部骨折发生率的主要决定因素,对于给定年龄的女性,其绝经年龄最多只有微弱的额外影响。请在文章后面查看编辑摘要。