Centre for Rheumatology, University College London, London, UK.
Rheumatology (Oxford). 2010 Jan;49(1):128-40. doi: 10.1093/rheumatology/kep346. Epub 2009 Nov 20.
To compare the efficacy and safety of mycophenolate mofetil (MMF) and intravenous cyclophosphamide (IVC) as induction treatment for lupus nephritis (LN), by race, ethnicity and geographical region.
A total of 370 patients with active Class III-V LN received MMF (target dose 3.0 g/day) or IVC (0.5-1.0 g/m(2)/month), plus tapered prednisone, for 24 weeks. Renal function, global disease activity, immunological complement (C3 and C4) and anti-dsDNA levels are the outcomes that were assessed in this study.
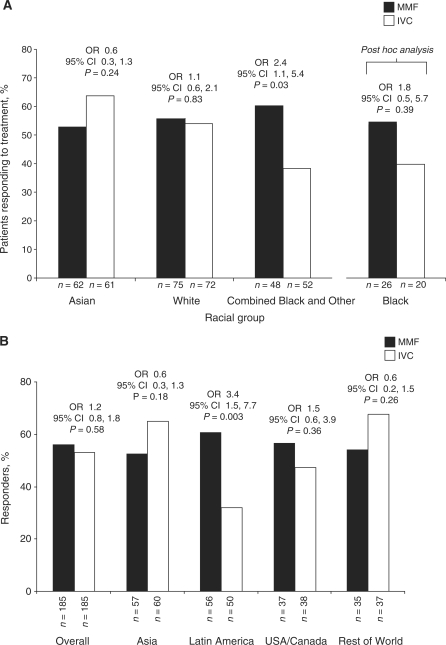
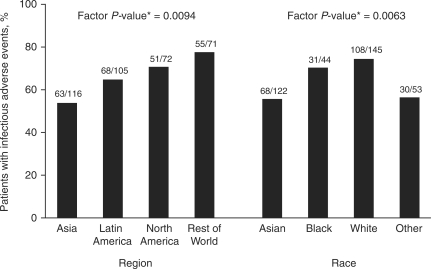
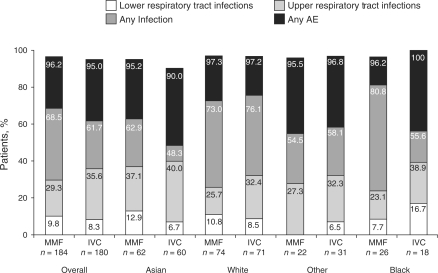
MMF was not superior to IVC as induction treatment (primary objective). There were important pre-specified interactions between treatment and race (P = 0.047) and treatment and region (P = 0.069) (primary endpoint). MMF and IVC response rates were similar for Asians (53.2 vs 63.9%; P = 0.24) and Whites (56.0 vs 54.2%; P = 0.83), but differed in the combined Other and Black group (60.4 vs 38.5%; P = 0.03). Fewer patients in the Black (40 vs 53.9%; P = 0.39) and Hispanic (38.8 vs 60.9%; P = 0.011) groups responded to IVC. Latin American patients had lower response to IVC (32 vs 60.7%; P = 0.003). Baseline disease characteristics were not predictive of response. The incidence of adverse events (AEs) was similar across groups. Serious AEs were slightly more prevalent among Asians.
MMF and IVC have similar efficacy overall to short-term induction therapy for LN. However, race, ethnicity and geographical region may affect treatment response; more Black and Hispanic patients responded to MMF than IVC. As these factors are inter-related, it is difficult to draw firm conclusions about their importance.
比较霉酚酸酯(MMF)与静脉注射环磷酰胺(IVC)作为狼疮肾炎(LN)诱导治疗的疗效和安全性,按种族、民族和地理区域进行比较。
共 370 例活动期 III-V 型 LN 患者接受 MMF(目标剂量 3.0 g/天)或 IVC(0.5-1.0 g/m2/月),加逐渐减量的泼尼松治疗 24 周。本研究评估了肾功能、总体疾病活动度、免疫补体(C3 和 C4)和抗 dsDNA 水平等结局。
MMF 作为诱导治疗并不优于 IVC(主要目标)。治疗与种族(P=0.047)和治疗与区域(P=0.069)之间存在重要的预先指定的交互作用(主要终点)。MMF 和 IVC 对亚洲人(53.2% vs 63.9%;P=0.24)和白人(56.0% vs 54.2%;P=0.83)的反应率相似,但在其他种族和黑人的组合中不同(60.4% vs 38.5%;P=0.03)。黑人(40% vs 53.9%;P=0.39)和西班牙裔(38.8% vs 60.9%;P=0.011)组中接受 IVC 治疗的患者较少。拉丁美洲患者对 IVC 的反应较低(32% vs 60.7%;P=0.003)。基线疾病特征对反应无预测作用。各组不良反应(AE)的发生率相似。亚洲人 AE 的发生率略高。
MMF 和 IVC 对 LN 的短期诱导治疗总体疗效相似。然而,种族、民族和地理区域可能影响治疗反应;更多的黑人患者和西班牙裔患者对 MMF 有反应,而不是 IVC。由于这些因素相互关联,因此很难对它们的重要性得出明确的结论。