Ludwig-Maximilians-University, Department of Cardiology, Grosshadern Campus, Munich, Germany.
BMC Cardiovasc Disord. 2009 Dec 11;9:54. doi: 10.1186/1471-2261-9-54.
Coronary artery anomalies (CAAs) are currently undergoing profound changes in understanding potentially pathophysiological mechanisms of disease. Aim of this study was to investigate the prevalence of anomalous origin and course of coronary arteries in consecutive symptomatic patients, who underwent cardiac 64-slice multidetector-row computed tomography angiography (MDCTA).
Imaging datasets of 748 consecutive symptomatic patients referred for cardiac MDCTA were analyzed and CAAs of origin and further vessel course were grouped according to a recently suggested classification scheme by Angelini et al.
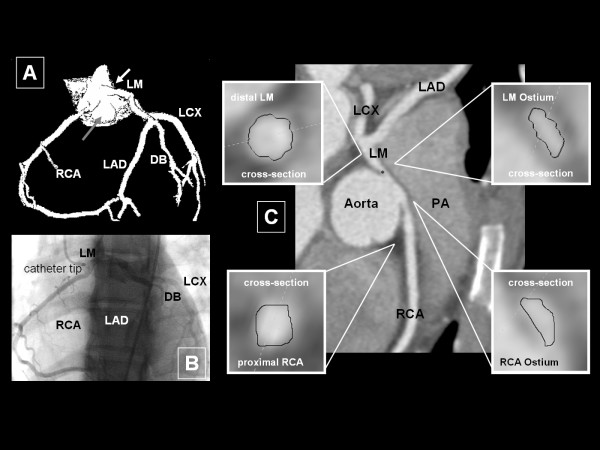
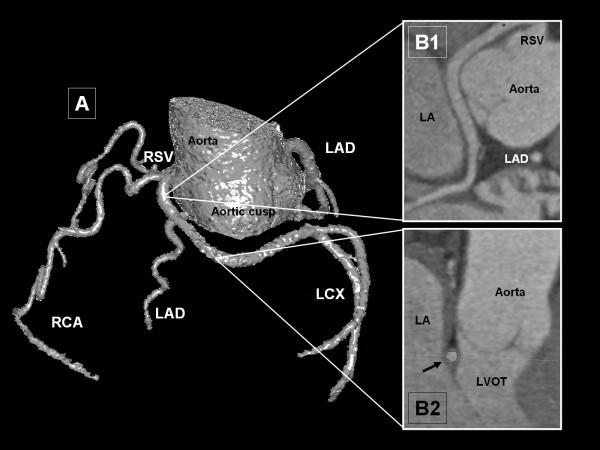
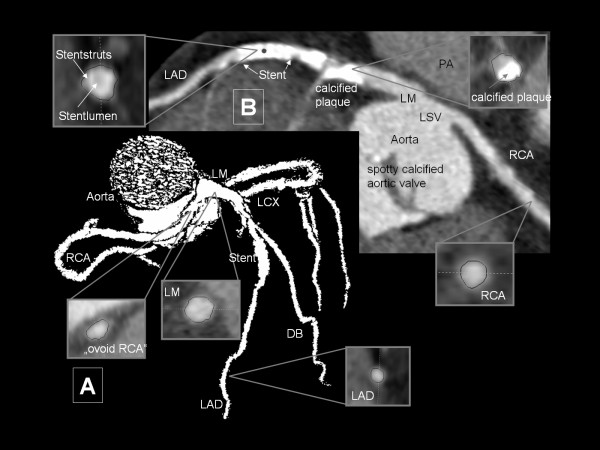
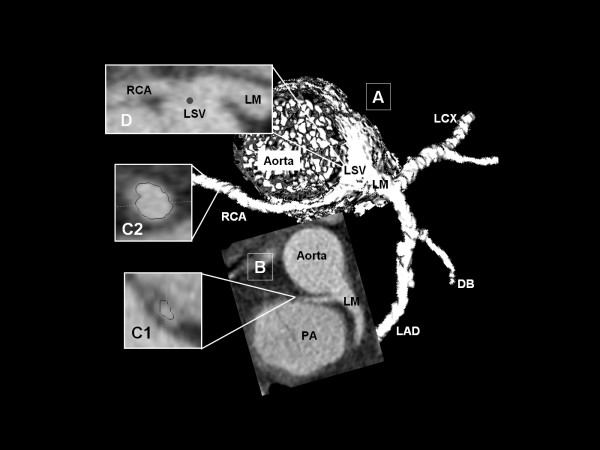
An overall of 17/748 patients (2.3%) showed CAA of origin and further vessel course. According to aforementioned classification scheme no Subgroup 1- (absent left main trunk) and Subgroup 2- (anomalous location of coronary ostium within aortic root or near proper aortic sinus of Valsalva) CAA were found. Subgroup 3 (anomalous location of coronary ostium outside normal "coronary" aortic sinuses) consisted of one patient with high anterior origin of both coronary arteries. The remaining 16 patients showed a coronary ostium at improper sinus (Subgroup 4). Latter group was subdivided into a right coronary artery arising from left anterior sinus with separate ostium (subgroup 4a; n = 7) and common ostium with left main coronary artery (subgroup 4b; n = 1). Subgroup 4c consisted of one patient with a single coronary artery arising from the right anterior sinus (RAS) without left circumflex coronary artery (LCX). In subgroup 4d, LCX arose from RAS (n = 7).
Prevalence of CAA of origin and further vessel course in a symptomatic consecutive patient population was similar to large angiographic series, although these patients do not reflect general population. However, our study supports the use of 64-slice MDCTA for the identification and definition of CAA.
冠状动脉异常(CAA)目前在理解疾病潜在病理生理机制方面正在发生深刻变化。本研究的目的是调查连续症状性患者中经心脏 64 层多排螺旋 CT 血管造影(MDCTA)检查的冠状动脉异常起源和走行的发生率。
对 748 例连续症状性患者的影像学资料进行分析,根据 Angelini 等人提出的分类方案,将起源和进一步血管走行的 CAA 进行分组。
共有 17/748 例(2.3%)患者存在起源和进一步血管走行的 CAA。根据上述分类方案,未发现第 1 亚组(左主干缺失)和第 2 亚组(冠状动脉开口异常位于主动脉根部或靠近正确的主动脉窦)的 CAA。第 3 亚组(冠状动脉开口异常位于正常“冠状动脉”主动脉窦之外)包括 1 例左右冠状动脉高位起源。其余 16 例患者存在冠状动脉开口位置不当(第 4 亚组)。后者亚组进一步分为左前窦发出的右冠状动脉(第 4a 亚组;n = 7)和与左主干冠状动脉共同开口(第 4b 亚组;n = 1)。第 4c 亚组包括 1 例单一冠状动脉起源于右前窦,无左回旋支冠状动脉(LCX)(n = 1)。第 4d 亚组,LCX 起源于 RAS(n = 7)。
在连续症状性患者人群中,CAA 的起源和进一步血管走行的发生率与大型血管造影系列相似,尽管这些患者不能反映一般人群。然而,我们的研究支持使用 64 层 MDCTA 来识别和定义 CAA。