Vaidyanathan Subramanian, Soni Bakul M, Singh Gurpreet, Hughes Peter L, Mansour Paul, Oo Tun
Spinal Injuries Unit, District General Hospital, Town Lane, Southport PR8 6PN, UK.
Cases J. 2009 Dec 22;2:9371. doi: 10.1186/1757-1626-2-9371.
In female patients with neuropathic bladder, the urethra is closed permanently in order to avoid urine leak. Then Benchekroun hydraulic ileal valve is attached to urinary bladder, thus providing a continent stoma for performing intermittent catheterisations.
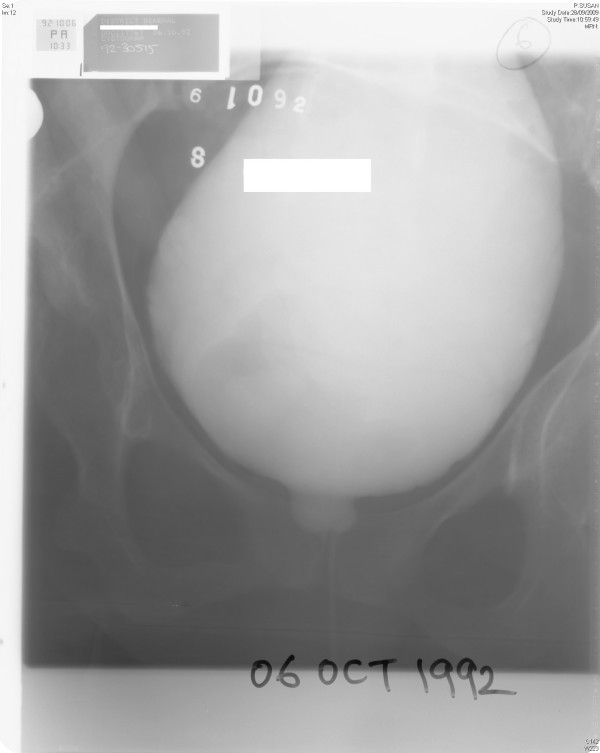
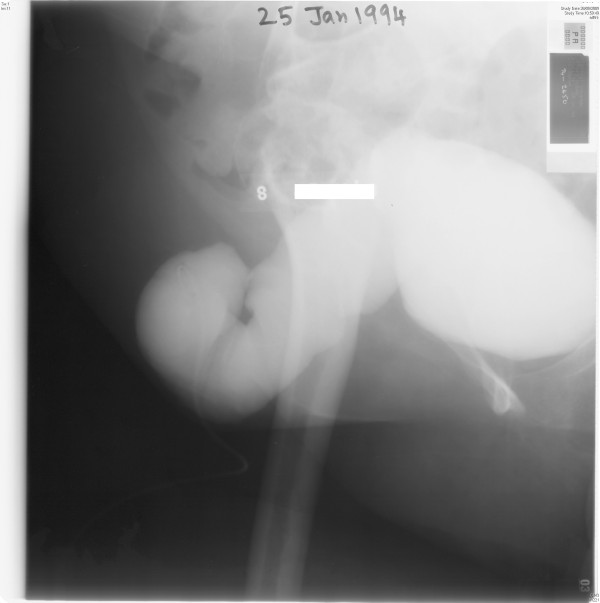
We present a female patient with spina bifida who underwent Benchekroun continent vesicostomy in 1993. This patient developed severe stenosis of Benchekroun stoma and stones in urinary bladder. Dilatation of stoma and vesicolithotomy were carried out in 1995. Vesical calculi recurred; suprapubic cystolithotomy was performed in 1999. In March 2000, catheterisation of stoma was not possible and emergency suprapubic cystostomy was done. In April 2000, endoscopy was attempted through Benchekroun stoma. It was not possible to insert ureterorenoscope beyond two inches. The track was completely blocked. In November 2001, X-ray of abdomen showed several vesical calculi; suprapubic cystolithotomy was performed. In March 2005, this patient developed pain in abdomen. X-ray of abdomen showed a large vesical calculus. In June 2005, suprapubic catheter was removed and a cystoscope was introduced in to the bladder. Then electrohydraulic lithotripsy was performed. In 2007, this patient was concerned about the increasing swelling in lower abdomen. Computed tomography of abdomen revealed midline, lower abdominal wall hernia, which contained several loops of small bowel and ileal cystoplasty. The large hernia was uncomfortable and tender on coughing, but did not cause obstructive bowel symptoms. Surgical repair of hernia was considered. But this patient would require alternative way of urinary diversion because the current location of suprapubic catheter would almost lead to infection of prosthetic material used in reconstruction of the anterior abdominal wall. After discussing risks of operative procedures with patient and her husband, it was decided not to proceed with surgery.
This case is a poignant reminder to spinal cord physicians that novel surgical techniques should be viewed cautiously, and patients should be informed of potential complications of surgical procedures some of which could be irreversible.
在患有神经源性膀胱的女性患者中,尿道需永久性闭合以避免尿液渗漏。然后将本谢克鲁恩液压回肠瓣连接至膀胱,从而提供一个可控造口以便进行间歇性导尿。
我们报告一名患有脊柱裂的女性患者,她于1993年接受了本谢克鲁恩可控膀胱造口术。该患者出现了本谢克鲁恩造口严重狭窄及膀胱结石。1995年进行了造口扩张及膀胱结石切除术。膀胱结石复发;1999年进行了耻骨上膀胱切开取石术。2000年3月,无法对造口进行导尿,遂进行了急诊耻骨上膀胱造瘘术。2000年4月,尝试通过本谢克鲁恩造口进行内镜检查。输尿管肾镜无法插入超过两英寸。通道完全堵塞。2001年11月,腹部X线显示多个膀胱结石;进行了耻骨上膀胱切开取石术。2005年3月,该患者出现腹痛。腹部X线显示一个大的膀胱结石。2005年6月,拔除耻骨上导尿管并将膀胱镜插入膀胱。然后进行了液电碎石术。2007年,该患者担心下腹部肿胀加剧。腹部计算机断层扫描显示中线、下腹壁疝,其中包含几段小肠和回肠膀胱扩大术。大疝在咳嗽时不舒服且有压痛,但未引起肠梗阻症状。考虑进行疝修补手术。但由于耻骨上导尿管的当前位置几乎会导致用于重建前腹壁的假体材料感染,该患者需要替代的尿液转流方式。在与患者及其丈夫讨论手术风险后,决定不进行手术。
该病例强烈提醒脊髓科医生,对于新的手术技术应谨慎看待,并且应告知患者手术可能存在一些潜在并发症,其中一些可能是不可逆的。