Psychiatric Research Centre of Northern Norway, University Hospital of North Norway, Tromsø, Norway.
Int J Ment Health Syst. 2010 Mar 31;4:5. doi: 10.1186/1752-4458-4-5.
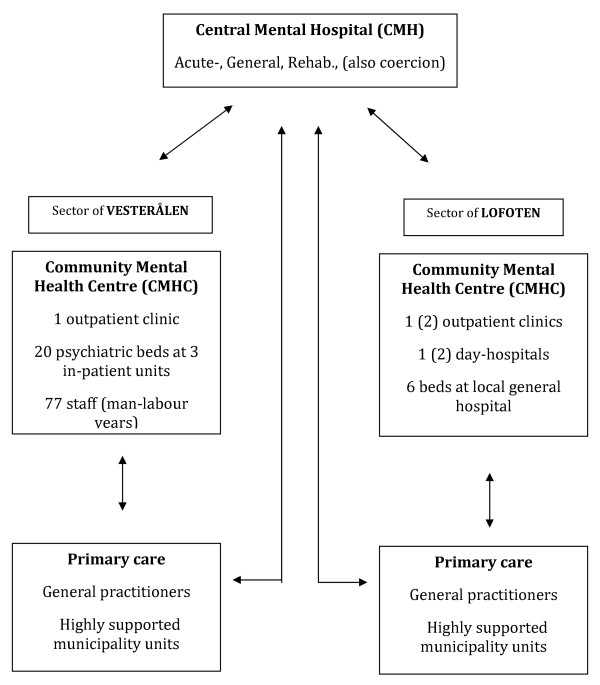
There are few reports on the effects of extensive decentralization of mental health services. We investigated the total patterns of utilization in a local-bed model and a central-bed model.
In a time-trend case-registry design, 7635 single treatment episodes, from the specialist and municipality services in 2003-2006, were linked to 2975 individual patients over all administrative levels. Patterns of utilization were analyzed by univariate comparisons and multivariate regressions.
Total treated prevalence was consistently higher for the central-bed system. Outpatient utilization increased markedly, in the central-bed system. Utilization of psychiatric beds decreased, only in the central-bed system. Utilization of highly supported municipality units increased in both systems. Total utilization of all types of services, showed an additive pattern in the local-bed system and a substitutional pattern in the central-bed system. Only severe diagnoses predicted inpatient admission in the central-bed system, whereas also anxiety-disorders and outpatient consultations predicted inpatient admission in the local-bed system. Characteristics of the inpatient populations changed markedly over time, in the local-bed system.
Geographical availability is not important as a filter in patients' pathway to inpatient care, and the association between distance to hospital and utilization of psychiatric beds may be an historical artefact. Under a public health-insurance system, local psychiatric personnel as gatekeepers for inpatient care may be of greater importance than the availability of local psychiatric beds. Specialist psychiatric beds and highly supported municipality units for people with mental health problems do not work together in terms of utilization. Outpatient and day-hospital services may be filters in the pathway to inpatient care, however this depends on the structure of the whole service-system. Local integration of psychiatric services may bring about additive, rather than substitutional patterns of total utilization. A large proportion of decentralized psychiatric beds may hinder the development of various local psychiatric services, with negative consequences for overall treated prevalence.
关于精神卫生服务广泛分散化的效果,鲜有报道。我们调查了本地床位模式和中央床位模式下的总利用情况。
采用时间趋势病例对照设计,将 2003-2006 年专家和市政服务的 7635 例单次治疗与所有行政级别的 2975 名患者进行了关联。通过单变量比较和多变量回归分析了利用模式。
中央床位系统的总治疗流行率始终较高。中央床位系统的门诊利用率显著增加。中央床位系统的精神病床位利用率下降,而本地床位系统的利用率增加。两种系统的高度支持市政单位的利用率均增加。在本地床位系统中,所有类型服务的总利用率呈附加模式,而在中央床位系统中呈替代模式。只有严重诊断在中央床位系统中预测住院,而焦虑障碍和门诊咨询也预测了本地床位系统中的住院。本地床位系统中住院人群的特征随时间发生了明显变化。
地理位置的可用性不是患者住院途径的重要筛选因素,而与医院的距离和精神病床位的利用之间的关系可能是历史遗留问题。在公共医疗保险制度下,作为住院治疗把关人的当地精神科人员可能比当地精神病床位的可用性更为重要。精神科专家床位和有精神健康问题的高度支持市政单位在利用方面并未协同工作。然而,门诊和日间医院服务可能是住院途径的筛选因素,但这取决于整个服务系统的结构。当地精神科服务的整合可能会带来总利用率的附加模式,而不是替代模式。大量分散的精神病床位可能会阻碍各种当地精神科服务的发展,从而对总体治疗流行率产生负面影响。