Qureshi Adnan I, Palesch Yuko Y, Martin Reneé, Novitzke Jill, Cruz-Flores Salvador, Ehtisham As'ad, Ezzeddine Mustapha A, Goldstein Joshua N, Hussein Haitham M, Suri M Fareed K, Tariq Nauman
Zeenat Qureshi Stroke Research Center, University of Minnesota, Minneapolis, MN 55455, USA.
Arch Neurol. 2010 May;67(5):570-6. doi: 10.1001/archneurol.2010.61.
Evidence indicates that systolic blood pressure (SBP) reduction may reduce hematoma expansion in patients with intracerebral hemorrhage (ICH) who are initially seen with acute hypertensive response.
To explore the relationship between different variables of SBP reduction and hematoma expansion, perihematomal edema, and 3-month outcome among patients with ICH.
Post hoc analysis of a traditional phase 1 dose-escalation multicenter prospective study.
Emergency departments and intensive care units.
Patients having ICH with an elevated SBP of at least 170 mm Hg who were seen within 6 hours of symptom onset.
Systolic blood pressure reduction using intravenous nicardipine hydrochloride targeting 3 tiers of sequentially escalating SBP reduction goals (170-199, 140-169, or 110-139 mm Hg).
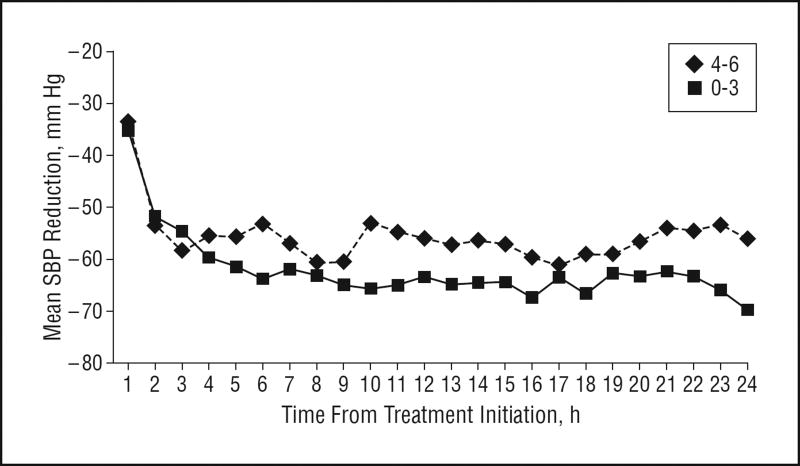
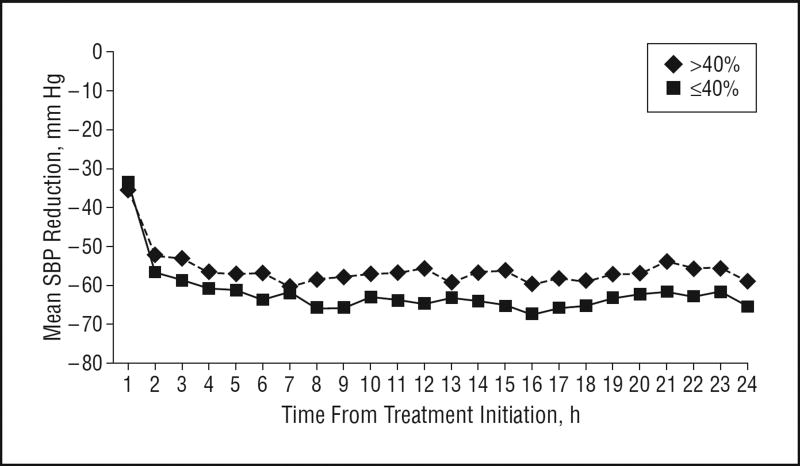
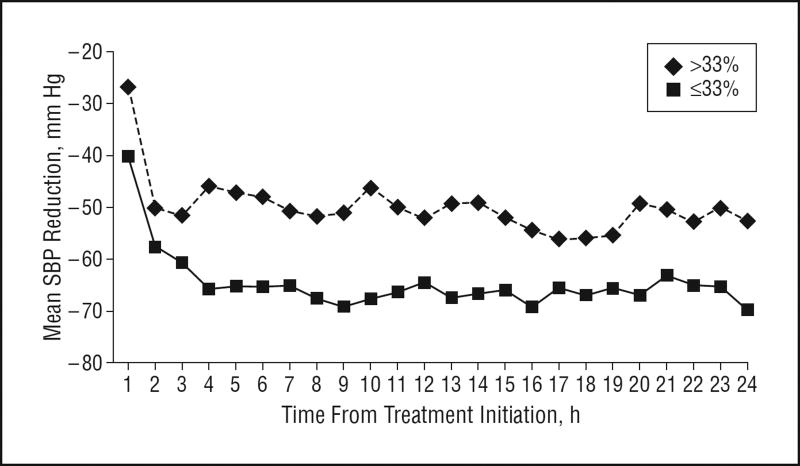
We evaluated the effect of SBP reduction (relative to initial SBP) on the following: hematoma expansion (defined as an increased intraparenchymal hemorrhage volume >33% on 24-hour vs baseline computed tomographic [CT] images), higher perihematomal edema ratio (defined as a >40% increased ratio of edema volume to hematoma volume on 24-hour vs baseline CT images), and poor 3-month outcome (defined as a modified Rankin scale score of 4-6).
Sixty patients (mean [SD] age, 62.0 [15.1] years; 34 men) were recruited (18, 20, and 22 patients in each of the 3 SBP reduction goal tiers). The median area under the curve (AUC) (calculated as the area between the hourly SBP measurements over 24 hours and the baseline SBP) was 1360 (minimum, 3643; maximum, 45) U. Comparing patients having less vs more aggressive SBP reduction based on 24-hour AUC analysis, frequencies were 32% vs 17% for hematoma expansion, 61% vs 40% for higher perihematomal edema ratio, and 46% vs 38% for poor 3-month outcome (P > .05 for all). The median SBP reductions were 54 mm Hg at 6 hours and 62 mm Hg at 6 hours from treatment initiation. Comparing patients having equal to or less vs more than the median SBP reduction at 2 hours, frequencies were 21% vs 31% for hematoma expansion, 42% vs 57% for higher perihematomal edema ratio, and 35% vs 48% for poor 3-month outcome (P > .05 for all).
We found no significant relationship between SBP reduction and any of the outcomes measured herein; however, the Antihypertensive Treatment of Acute Cerebral Hemorrhage study was primarily a safety study and was not powered for such end points. The consistent favorable direction of these associations supports further studies with an adequately powered randomized controlled design to evaluate the efficacy of aggressive pharmacologic SBP reduction.
有证据表明,收缩压(SBP)降低可能会减少脑出血(ICH)患者的血肿扩大,这些患者最初表现为急性高血压反应。
探讨脑出血患者SBP降低的不同变量与血肿扩大、血肿周围水肿及3个月预后之间的关系。
对一项传统的1期剂量递增多中心前瞻性研究进行事后分析。
急诊科和重症监护病房。
症状发作6小时内就诊的脑出血患者,其SBP至少升高至170 mmHg。
使用静脉注射盐酸尼卡地平降低收缩压,目标是3个依次递增的SBP降低目标水平(170 - 199、140 - 169或110 - 139 mmHg)。
我们评估了SBP降低(相对于初始SBP)对以下方面的影响:血肿扩大(定义为24小时时脑实质内出血体积较基线计算机断层扫描[CT]图像增加>33%)、较高的血肿周围水肿比率(定义为24小时时水肿体积与血肿体积之比相对于基线CT图像增加>40%)以及3个月预后不良(定义为改良Rankin量表评分为4 - 6分)。
招募了60例患者(平均[标准差]年龄,62.0 [15.1]岁;34例男性)(3个SBP降低目标水平组分别为18、20和22例患者)。曲线下面积(AUC)中位数(计算为24小时内每小时SBP测量值与基线SBP之间的面积)为1360(最小值,3643;最大值,45)U。根据24小时AUC分析比较SBP降低程度较小与较大的患者,血肿扩大的发生率分别为32%和17%,较高血肿周围水肿比率的发生率分别为61%和40%,3个月预后不良的发生率分别为46%和38%(所有P>0.05)。治疗开始后6小时SBP降低中位数为54 mmHg,6小时时为62 mmHg。比较2小时时SBP降低等于或低于中位数与高于中位数的患者,血肿扩大的发生率分别为21%和31%,较高血肿周围水肿比率的发生率分别为42%和57%,3个月预后不良的发生率分别为35%和48%(所有P>0.05)。
我们发现SBP降低与本文测量的任何结局之间均无显著关系;然而,急性脑出血的降压治疗研究主要是一项安全性研究,未针对此类终点进行足够的效能分析。这些关联一致的有利方向支持进一步开展具有足够效能的随机对照设计研究,以评估积极的药物性SBP降低的疗效。