Department of Urology, Institute of Clinical Sciences, Sahlgrenska Academy at University of Göteborg, Sweden.
Lancet Oncol. 2010 Aug;11(8):725-32. doi: 10.1016/S1470-2045(10)70146-7. Epub 2010 Jul 2.
Prostate cancer is one of the leading causes of death from malignant disease among men in the developed world. One strategy to decrease the risk of death from this disease is screening with prostate-specific antigen (PSA); however, the extent of benefit and harm with such screening is under continuous debate.
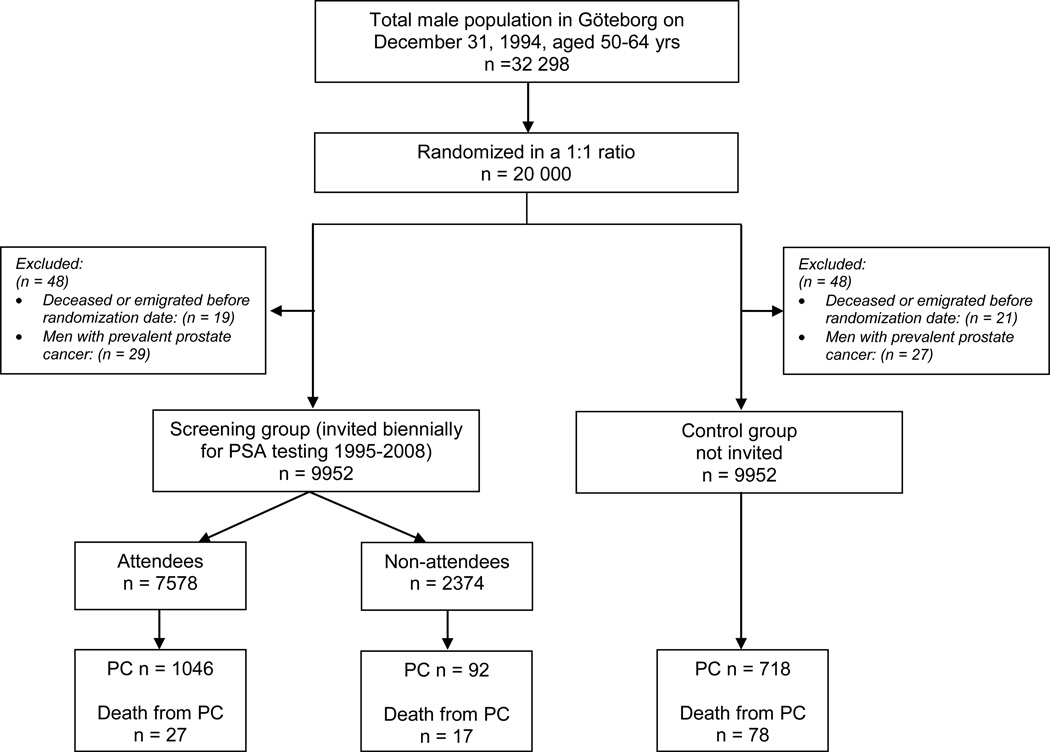
In December, 1994, 20,000 men born between 1930 and 1944, randomly sampled from the population register, were randomised by computer in a 1:1 ratio to either a screening group invited for PSA testing every 2 years (n=10,000) or to a control group not invited (n=10,000). Men in the screening group were invited up to the upper age limit (median 69, range 67-71 years) and only men with raised PSA concentrations were offered additional tests such as digital rectal examination and prostate biopsies. The primary endpoint was prostate-cancer specific mortality, analysed according to the intention-to-screen principle. The study is ongoing, with men who have not reached the upper age limit invited for PSA testing. This is the first planned report on cumulative prostate-cancer incidence and mortality calculated up to Dec 31, 2008. This study is registered as an International Standard Randomised Controlled Trial ISRCTN54449243.
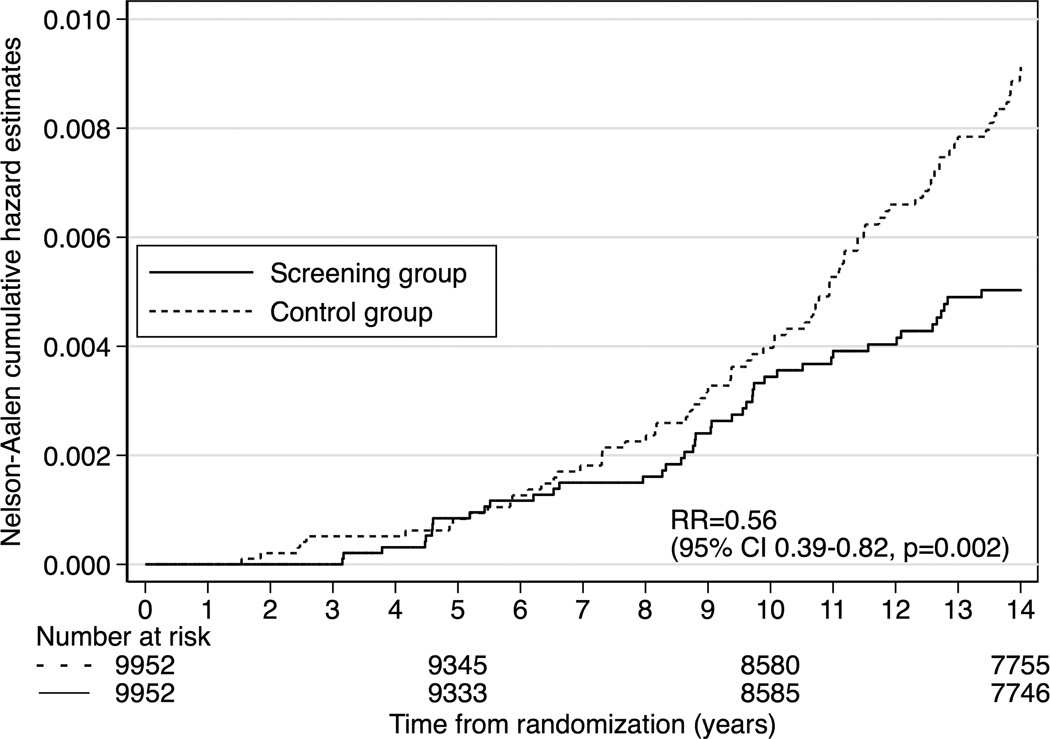
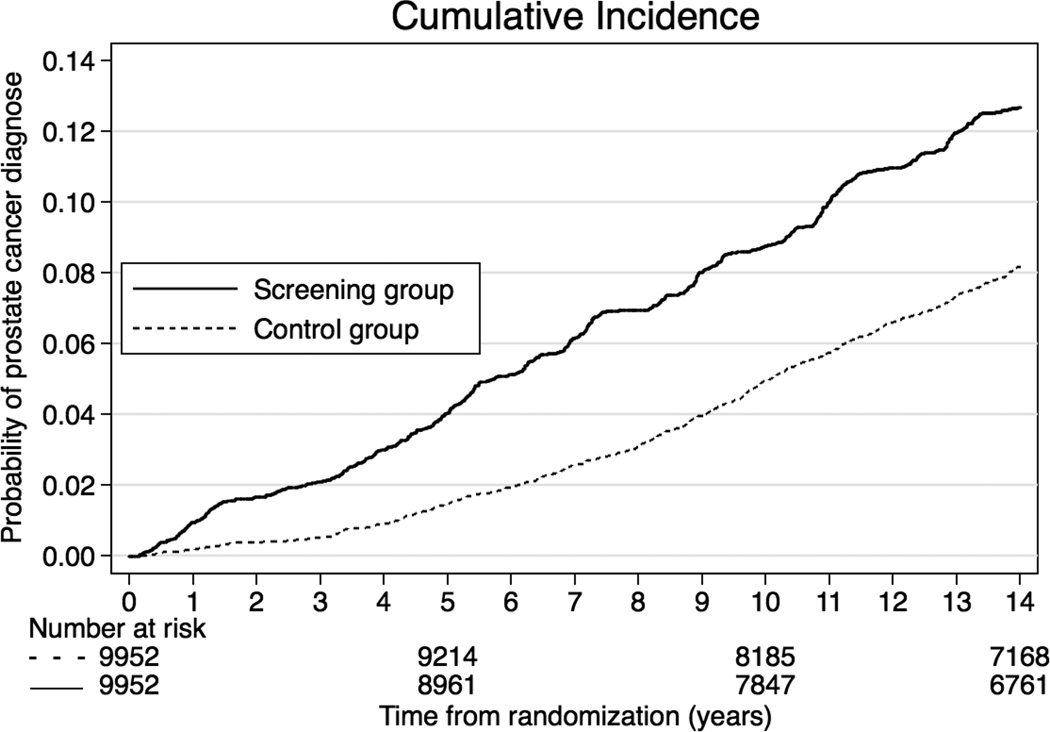
In each group, 48 men were excluded from the analysis because of death or emigration before the randomisation date, or prevalent prostate cancer. In men randomised to screening, 7578 (76%) of 9952 attended at least once. During a median follow-up of 14 years, 1138 men in the screening group and 718 in the control group were diagnosed with prostate cancer, resulting in a cumulative prostate-cancer incidence of 12.7% in the screening group and 8.2% in the control group (hazard ratio 1.64; 95% CI 1.50-1.80; p<0.0001). The absolute cumulative risk reduction of death from prostate cancer at 14 years was 0.40% (95% CI 0.17-0.64), from 0.90% in the control group to 0.50% in the screening group. The rate ratio for death from prostate cancer was 0.56 (95% CI 0.39-0.82; p=0.002) in the screening compared with the control group. The rate ratio of death from prostate cancer for attendees compared with the control group was 0.44 (95% CI 0.28-0.68; p=0.0002). Overall, 293 (95% CI 177-799) men needed to be invited for screening and 12 to be diagnosed to prevent one prostate cancer death.
This study shows that prostate cancer mortality was reduced almost by half over 14 years. However, the risk of over-diagnosis is substantial and the number needed to treat is at least as high as in breast-cancer screening programmes. The benefit of prostate-cancer screening compares favourably to other cancer screening programs.
The Swedish Cancer Society, the Swedish Research Council, and the National Cancer Institute.
在发达国家,前列腺癌是男性恶性肿瘤死亡的主要原因之一。降低死于这种疾病风险的一种策略是使用前列腺特异性抗原(PSA)进行筛查;然而,这种筛查的益处和危害程度仍在不断争论中。
1994 年 12 月,从人口登记册中随机抽取 20,000 名出生于 1930 年至 1944 年之间的男性,通过计算机以 1:1 的比例随机分配到筛查组(10,000 人)或对照组(10,000 人)。筛查组的男性每两年接受一次 PSA 检测(n=10,000),而对照组则不接受邀请(n=10,000)。筛查组的男性邀请至最高年龄限制(中位数 69 岁,范围 67-71 岁),只有 PSA 浓度升高的男性才会接受额外的检查,如直肠指检和前列腺活检。主要终点是前列腺癌特异性死亡率,按照意向性筛查原则进行分析。该研究正在进行中,尚未达到最高年龄限制的男性被邀请进行 PSA 检测。这是首次计划报告截至 2008 年 12 月 31 日的累积前列腺癌发病率和死亡率。该研究在国际随机对照试验注册处(ISRCTN54449243)注册。
在每组中,有 48 名男性因死亡或移民或在随机分组日期前患有前列腺癌而被排除在分析之外。在接受筛查的男性中,有 9952 人中有 7578 人至少参加过一次。在中位数为 14 年的随访期间,筛查组中有 1138 名男性和对照组中有 718 名男性被诊断为前列腺癌,导致筛查组的累积前列腺癌发病率为 12.7%,对照组为 8.2%(风险比 1.64;95%CI 1.50-1.80;p<0.0001)。在 14 年时,前列腺癌死亡的累积风险降低了 0.40%(95%CI 0.17-0.64),从对照组的 0.90%降至筛查组的 0.50%。与对照组相比,筛查组前列腺癌死亡率的比率为 0.56(95%CI 0.39-0.82;p=0.002)。与对照组相比,参加筛查的男性前列腺癌死亡率的比率为 0.44(95%CI 0.28-0.68;p=0.0002)。总体而言,需要邀请 293 名(95%CI 177-799)男性进行筛查,需要诊断 12 名男性才能预防 1 例前列腺癌死亡。
这项研究表明,14 年来前列腺癌死亡率降低了近一半。然而,过度诊断的风险很大,需要治疗的人数至少与乳腺癌筛查计划一样高。前列腺癌筛查的益处与其他癌症筛查计划相当。
瑞典癌症协会、瑞典研究理事会和国家癌症研究所。