Department of Obstetrics and Gynecology, Meharry Medical College, Nashville, TN 37208-3599, USA.
Int J Environ Res Public Health. 2010 May;7(5):2033-44. doi: 10.3390/ijerph7052033. Epub 2010 Apr 28.
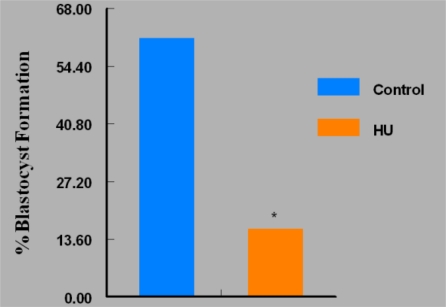
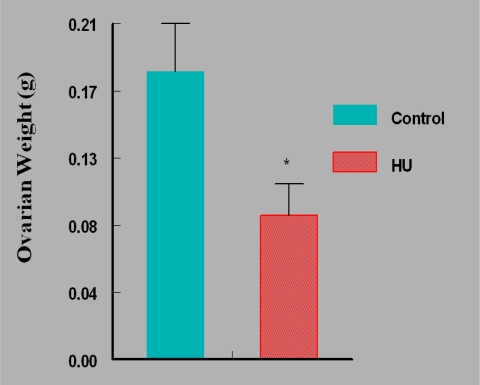
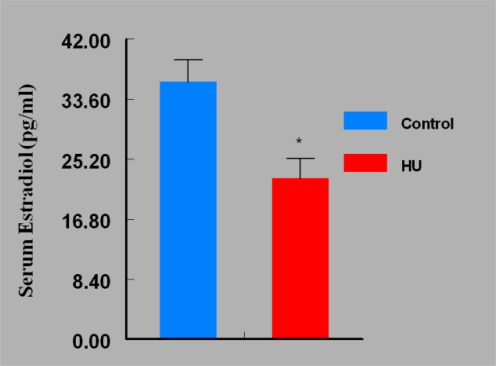
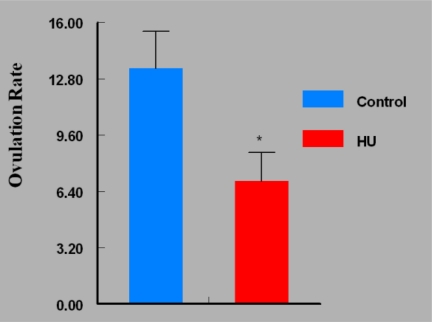
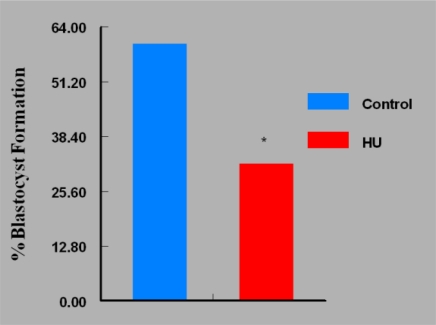
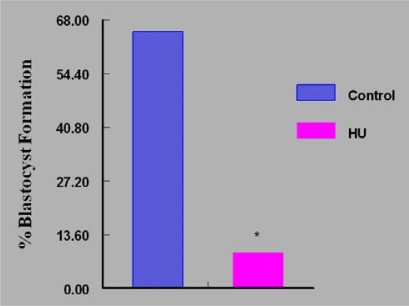
Women are advised not to attempt pregnancy while on hydroxyurea (HU) due to the teratogenic effects of this agent, based on results obtained from animal studies. Several case reports suggest that HU may have minimal or no teratogenic effects on the developing human fetus. Fourteen cases of HU therapy in pregnant patients diagnosed with acute or chronic myelogenous leukemia, primary thrombocythemia, or sickle cell disease (SCD) have been reported. Three pregnancies were terminated by elective abortion; 1 woman developed eclampsia and delivered a phenotypically normal stillborn infant. All other patients delivered live, healthy infants without congenital anomalies. We contend that case studies such as these have too few patients and cannot effectively address the adverse effect of HU on preimplantation embryo or fetuses. The objective of this study was to assess the risks associated with a clinically relevant dose of HU used for the treatment of SCD, on ovulation rate and embryo development, using adult C57BL/6J female mice as a model. In Experiment 1, adult female mice were randomly assigned to a treatment or a control group (N = 20/group). Treatment consisted of oral HU (30 mg/kg) for 28 days; while control mice received saline (HU vehicle). Five days to the cessation of HU dosing, all mice were subjected to folliculogenesis induction with pregnant mare serum gonadotropin (PMSG). Five mice/group were anesthetized at 48 hours post PMSG to facilitate blood collection via cardiac puncture for estradiol-17beta (E(2)) measurement by RIA. Ovulation was induced in the remaining mice at 48 hours post PMSG with human chorionic gonadotropin (hCG) and immediately caged with adult males for mating. Five plugged female mice/group were sacrificed for the determination of ovulation rate. The remaining mated mice were sacrificed about 26 hours post hCG, ovaries excised and weighed and embryos harvested and cultured in Whitten's medium (WM) supplemented with CZBt. In Experiments 2 and 3, (N = 10/Experiment) folliculogenesis and ovulation were induced in untreated mice followed by mating. Recovered embryos were either exposed continuously (Experiment 2) or intermittently (Experiment 3) to bioavailable HU (18 microg HU/mL of WM + CZBt) or WM + CZBt only (control). Treated mice sustained decreased ovarian wt, ovulation rate and circulating E(2) compared with controls (P < 0.05). Fewer embryos retrieved from HU-treated mice developed to blastocyst stage (32%) compared with those from controls (60%; P < 0.05). Furthermore, continuous or intermittent in vitro exposures of embryos to HU also resulted in reduced development to blastocyst stage (continuous HU, 9 vs. control, 63%; P < 0.05; intermittent HU, 20 vs. control, 62%; P < 0.05) with embryos exposed continuously to HU in vitro fairing worse. Even though HU is well tolerated, our data suggest that it compromises folliculogenesis and the ability of generated embryos to develop. Therefore, designed studies with larger numbers of patients receiving HU during pregnancy, with longer follow-up of exposed children and more careful assessment of embryo/fetotoxic effects, are required before this agent can be promoted as safe in pregnancy.
建议女性在服用羟基脲(HU)期间不要尝试怀孕,因为这种药物的致畸作用,这是基于动物研究的结果。一些病例报告表明,HU 对发育中的人类胎儿可能具有最小或没有致畸作用。已经报道了 14 例在怀孕患者中使用 HU 治疗急性或慢性髓性白血病、原发性血小板增多症或镰状细胞病(SCD)的病例。3 例妊娠因选择性流产终止;1 例妇女发生子痫并分娩出表型正常的死胎。所有其他患者均分娩出活产、健康的婴儿,无先天畸形。我们认为,像这样的病例研究患者太少,无法有效评估 HU 对着床前胚胎或胎儿的不良影响。本研究的目的是评估使用临床相关剂量的 HU 治疗 SCD 对排卵率和胚胎发育的相关风险,使用成年 C57BL/6J 雌性小鼠作为模型。在实验 1 中,成年雌性小鼠被随机分配到治疗组或对照组(每组 20 只)。治疗组接受 28 天的口服 HU(30mg/kg);而对照组小鼠给予生理盐水(HU 载体)。在停止 HU 给药 5 天后,所有小鼠均接受孕马血清促性腺激素(PMSG)诱导卵泡发生。每组 5 只小鼠在 PMSG 后 48 小时麻醉,通过心脏穿刺采集血液,用于放射免疫分析(RIA)测量雌二醇-17β(E2)。在 PMSG 后 48 小时,用人绒毛膜促性腺激素(hCG)诱导剩余的小鼠排卵,并立即与成年雄性小鼠交配。每组 5 只配种的雌性小鼠被处死,以确定排卵率。其余交配的小鼠在 hCG 后约 26 小时处死,取出卵巢称重,并采集胚胎在 Whitten 培养基(WM)中培养,补充 CZBt。在实验 2 和实验 3 中,(每组 10 只)未处理的小鼠诱导卵泡发生和排卵,然后交配。回收的胚胎连续(实验 2)或间歇(实验 3)暴露于生物可利用的 HU(18μg HU/mL 的 WM+CZBt)或 WM+CZBt(对照)。与对照组相比,接受 HU 治疗的小鼠卵巢重量、排卵率和循环 E2 降低(P<0.05)。与对照组(60%;P<0.05)相比,从 HU 处理的小鼠中回收的胚胎发育到囊胚阶段的数量较少(32%)。此外,胚胎连续或间歇暴露于 HU 体外也导致发育到囊胚阶段的数量减少(连续 HU,9 个,对照,63%;P<0.05;间歇 HU,20 个,对照,62%;P<0.05),连续暴露于 HU 体外的胚胎情况更糟。尽管 HU 耐受性良好,但我们的数据表明,它会损害卵泡发生和生成胚胎的发育能力。因此,在将这种药物推广为妊娠安全之前,需要进行设计良好的研究,在怀孕期间有更多数量的患者接受 HU 治疗,对暴露的儿童进行更长时间的随访,并更仔细地评估胚胎/胎儿毒性作用。