Department of Cardiology, Erasmus MC, Rotterdam, the Netherlands.
Europace. 2011 Jan;13(1):62-9. doi: 10.1093/europace/euq328. Epub 2010 Sep 10.
Comorbidity, such as myocardial infarction, diabetes, and renal failure, plays a pivotal role in the prognosis of a patient with arrhythmias. However, data on the prognostic impact of comorbiditiy in heart failure patients with cardiac resynchronization therapy and defibrillation (CRT-D) are scarce. The purpose of this study was to determine the impact of comorbidity on survival in CRT-D patients.
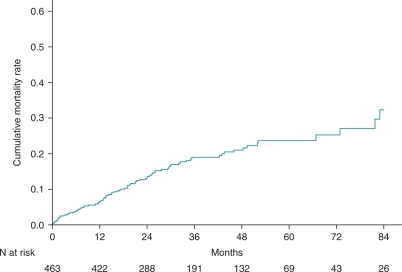
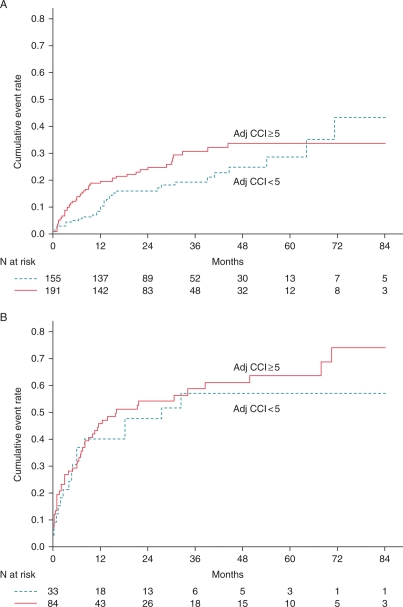
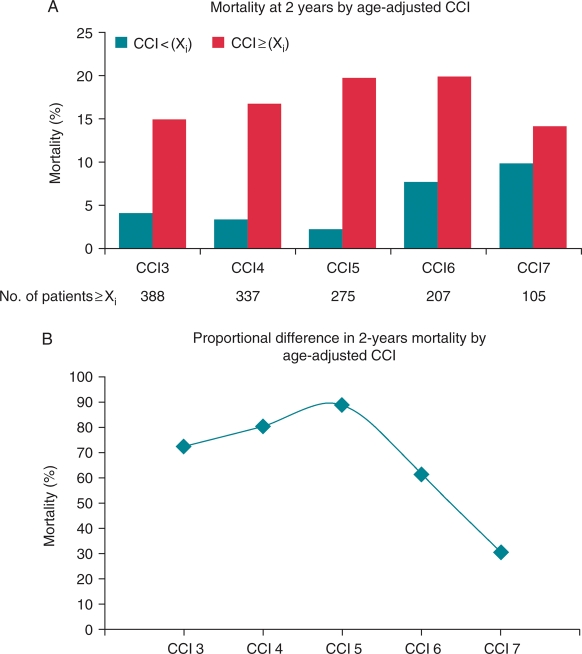
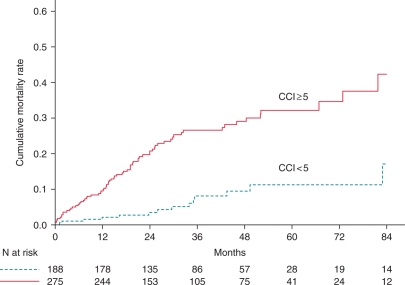
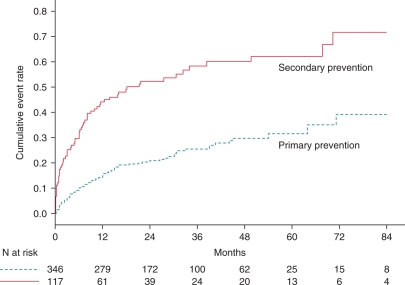
The study population consisted of 463 heart failure patients who received a CRT-D between 1999 and 2008 in Rotterdam and Basel. The Charlson comorbidity index (CCI) is often used as an adjusting variable in prognostic models. The Cox proportional hazards analysis was performed to determine the independent effect of comorbidity on survival. During a median follow-up of 30.5 months, 85 patients died. Mortality rates at 1 and 7 years were 6.3 and 32.3%. Cumulative incidence of implantable cardioverter defibrillator (ICD) therapy at 7 years was 50%, and death without ICD therapy was observed in 9% of patients. At least three comorbid conditions were observed in 81% of patients. Patients who died had a higher CCI score compared with those who survived (3.9 ± 1.5 vs. 2.9 ± 1.5; P < 0.001). An age-adjusted CCI score ≥ 5 was a predictor of mortality (hazard ratio 3.69, 95% CI 2.06-6.60; P < 0.001) independent from indication for ICD therapy, and from ICD interventions during the clinical course.
Comorbidity is often present in heart failure patients, and a high comorbidity burden was a significant predictor of mortality in CRT-D recipients. Comorbidity cannot predict appropriate ICD therapy. Death without prior ICD therapy occurs in a minor proportion of patients.
合并症(如心肌梗死、糖尿病和肾衰竭)对心律失常患者的预后起着关键作用。然而,关于心力衰竭患者心脏再同步治疗和除颤(CRT-D)合并症对预后影响的数据却很少。本研究旨在确定合并症对 CRT-D 患者生存的影响。
该研究人群包括 1999 年至 2008 年间在鹿特丹和巴塞尔接受 CRT-D 的 463 例心力衰竭患者。Charlson 合并症指数(CCI)常用于预后模型的调整变量。采用 Cox 比例风险分析确定合并症对生存的独立影响。在中位随访 30.5 个月期间,有 85 例患者死亡。1 年和 7 年的死亡率分别为 6.3%和 32.3%。7 年时植入式心脏复律除颤器(ICD)治疗的累积发生率为 50%,且有 9%的患者在未接受 ICD 治疗的情况下死亡。81%的患者至少有三种合并症。与存活患者相比,死亡患者的 CCI 评分更高(3.9 ± 1.5 比 2.9 ± 1.5;P < 0.001)。年龄调整后的 CCI 评分≥5 是死亡率的预测因素(风险比 3.69,95%CI 2.06-6.60;P < 0.001),独立于 ICD 治疗的指征,以及在临床过程中的 ICD 干预。
心力衰竭患者常合并多种疾病,高合并症负担是 CRT-D 患者死亡的重要预测因素。合并症不能预测适当的 ICD 治疗。在没有事先进行 ICD 治疗的情况下,死亡的患者比例较小。