Omerovic Elmir, Råmunddal Truls, Albertsson Per, Holmberg Mikael, Hallgren Per, Boren Jan, Grip Lars, Matejka Göran
Department of Cardiology, Sahlgrenska University Hospital, Gothenburg, Sweden.
Vasc Health Risk Manag. 2010 Sep 7;6:657-63. doi: 10.2147/vhrm.s8856.
The aim of this study was to evaluate the effect of levosimendan on mortality in cardiogenic shock (CS) after ST elevation myocardial infarction (STEMI).
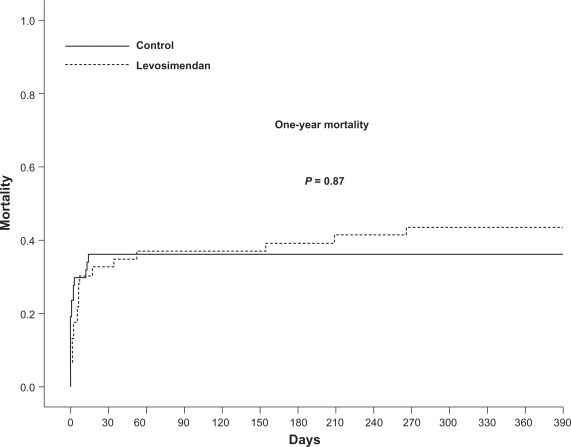
Data were obtained prospectively from the SCAAR (Swedish Coronary Angiography and Angioplasty Register) and the RIKS-HIA (Register of Information and Knowledge about Swedish Heart Intensive Care Admissions) about 94 consecutive patients with CS due to STEMI. Patients were classified into levosimendan-mandatory and levosimendan-contraindicated cohorts. Inotropic support with levosimendan was mandatory in all patients between January 2004 and December 2005 (n = 46). After the SURVIVE and REVIVE II studies were presented, levosimendan was considered contraindicated and was not used in consecutive patients between December 2005 and December 2006 (n = 48). The cohorts were similar with respect to pre-treatment characteristics and concomitant medications. There was no difference in the incidence of new-onset atrial fibrillation, in-hospital cardiac arrest and length of stay at the coronary care unit. There was no difference in adjusted mortality at 30 days and at one year.
The use of levosimendan neither improves nor worsens mortality in patients with CS due to STEMI. Well-designed randomized clinical trials are needed to define the role of inotropic therapy in the treatment of CS.
本研究旨在评估左西孟旦对ST段抬高型心肌梗死(STEMI)后心源性休克(CS)患者死亡率的影响。
前瞻性地从瑞典冠状动脉造影和血管成形术登记处(SCAAR)以及瑞典心脏重症监护入院信息与知识登记处(RIKS-HIA)获取了94例因STEMI导致CS的连续患者的数据。患者被分为左西孟旦强制使用组和左西孟旦禁忌组。在2004年1月至2005年12月期间,所有患者(n = 46)均强制使用左西孟旦进行正性肌力支持。在公布SURVIVE和REVIVE II研究结果后,左西孟旦被视为禁忌,在2005年12月至2006年12月期间的连续患者中未使用(n = 48)。两组在治疗前特征和伴随用药方面相似。新发房颤、院内心脏骤停发生率以及在冠心病监护病房的住院时间均无差异。30天和1年时的校正死亡率也无差异。
对于因STEMI导致CS的患者,使用左西孟旦既不会改善也不会恶化死亡率。需要设计良好的随机临床试验来确定正性肌力治疗在CS治疗中的作用。