Department of Surgery, Division of Cardiothoracic Surgery, Washington University School of Medicine, St. Louis, MO 63110, USA.
Ann Thorac Surg. 2010 Oct;90(4):1094-101. doi: 10.1016/j.athoracsur.2010.06.009.
Primary graft dysfunction (PGD) is a known risk factor for bronchiolitis obliterans syndrome (BOS) after lung transplantation. Here, we report that preformed antibodies to self-antigens increase PGD risk and promote BOS.
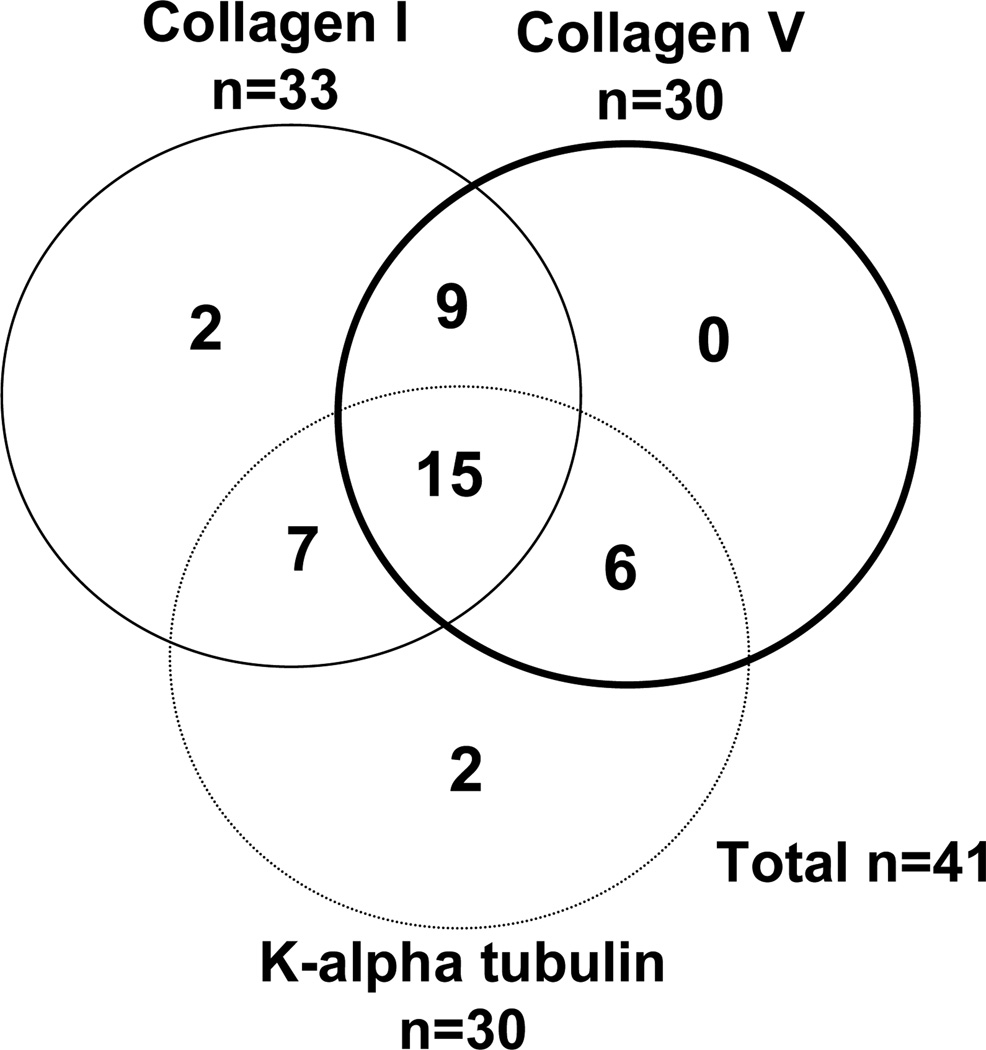
Adult lung transplant recipients (n = 142) were included in the study. Primary graft dysfunction and BOS were diagnosed based on International Society for Heart and Lung Transplantation guidelines. Antibodies to self-antigens k-alpha-1 tubulin, collagen type V, and collagen I were quantitated using standardized enzyme-linked immunosorbent assays, and cytokines were analyzed using Luminex immunoassays (Biosource International, Camirillo, CA). Human leukocyte antigen (HLA) antibodies were measured using Flow-PRA (One Lambda, Canoga Park, CA).
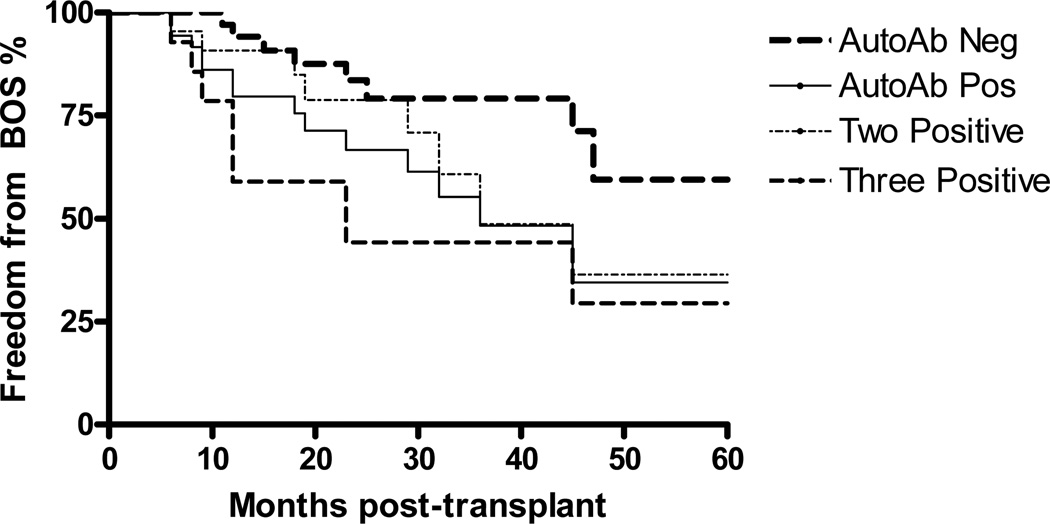
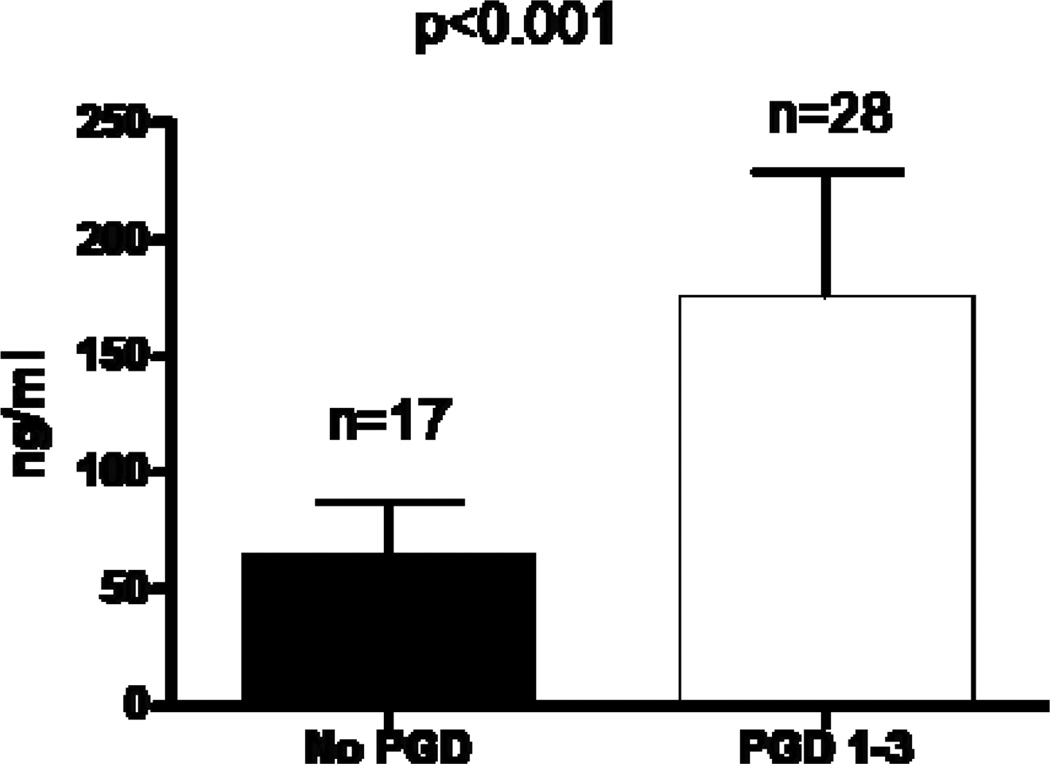
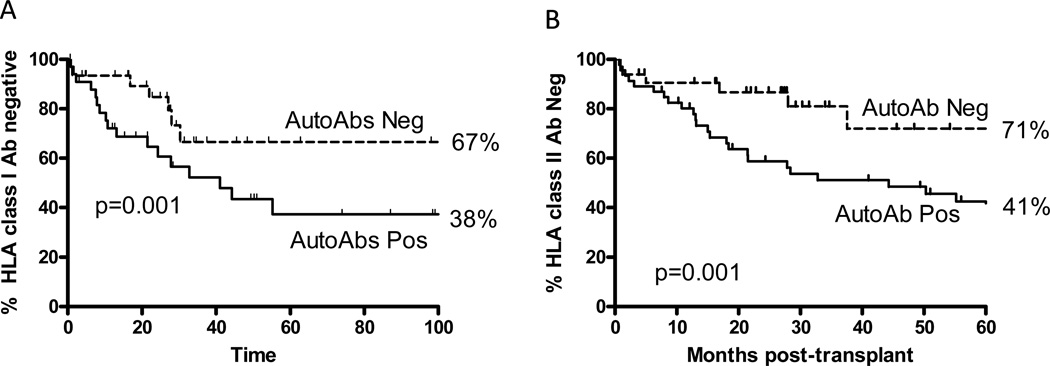
Lung transplant recipients with pretransplant antibodies to self-antigens had increased risk of PGD (odds ratio 3.09, 95% confidence interval: 1.2 to 8.1, p = 0.02) compared with recipients without. Conversely, in patients with PGD, 34.7% were positive for pretransplant antibodies whereas in the PGD negative group, only 14.6% had antibodies (p = 0.03). Antibody positive patients demonstrated high levels of proinflammatory cytokines interleukin (IL)-1β (2.1-fold increase), IL-2 (3.0), IL-12 (2.5), IL-15 (3.0), and chemokines interferon-inducible protein-10 (3.9) and monocyte chemotactic protein-1 (3.1; p < 0.01 for all). On 5-year follow-up, patients without antibodies showed greater freedom from development of HLA antibodies compared with patients who had antibodies (class I: 67% versus 38%, p = 0.001; class II: 71% versus 41%, p < 0.001). Patients with pretransplant antibodies were found to have an independent relative risk of 2.3 (95% confidence interval: 1.7 to 4.5, p = 0.009) for developing BOS.
Presence of antibodies to self-antigens pretransplant increases the risk of PGD immediately after transplant period and BOS on long-term follow-up. Primary graft dysfunction is associated with an inflammatory cascade that augments the alloimmune (anti-HLA) response that predisposes to BOS.
原发性移植物功能障碍(PGD)是肺移植后发生闭塞性细支气管炎综合征(BOS)的已知危险因素。在这里,我们报告说,针对自身抗原的预先形成的抗体增加了 PGD 的风险,并促进了 BOS 的发生。
纳入了 142 名成人肺移植受者进行研究。根据国际心肺移植协会的指南诊断原发性移植物功能障碍和 BOS。使用标准化酶联免疫吸附测定法定量检测针对自身抗原 k-α-1 微管蛋白、胶原类型 V 和胶原 I 的抗体,并使用 Luminex 免疫测定法(Biosource International,Camirillo,CA)分析细胞因子。使用 Flow-PRA(One Lambda,Canoga Park,CA)测量人类白细胞抗原(HLA)抗体。
与无抗体的受者相比,移植前存在针对自身抗原抗体的肺移植受者发生 PGD 的风险增加(优势比 3.09,95%置信区间:1.2 至 8.1,p=0.02)。相反,在 PGD 患者中,34.7%为移植前抗体阳性,而在 PGD 阴性组中,只有 14.6%有抗体(p=0.03)。抗体阳性患者表现出高水平的促炎细胞因子白细胞介素(IL)-1β(增加 2.1 倍)、IL-2(3.0)、IL-12(2.5)、IL-15(3.0)和趋化因子干扰素诱导蛋白-10(3.9)和单核细胞趋化蛋白-1(3.1;所有 p<0.01)。在 5 年的随访中,无抗体的患者与有抗体的患者相比,发展 HLA 抗体的自由度更大(I 类:67%对 38%,p=0.001;II 类:71%对 41%,p<0.001)。研究发现,移植前存在抗体的患者发生 BOS 的独立相对风险为 2.3(95%置信区间:1.7 至 4.5,p=0.009)。
移植前针对自身抗原的抗体的存在增加了移植后立即发生 PGD 和长期随访时发生 BOS 的风险。原发性移植物功能障碍与炎症级联反应相关,该级联反应增强了有利于 BOS 的同种免疫(抗 HLA)反应。