Department of Medical Oncology, Regina Elena National Cancer Institute, Roma, Italy.
BMC Cancer. 2010 Dec 9;10:675. doi: 10.1186/1471-2407-10-675.
Hormone therapy plus radiotherapy significantly decreases recurrences and mortality of patients affected by locally advanced prostate cancer. In order to determine if difference exists according to the hormonal treatment duration, a literature-based meta-analysis was performed.
Relative risks (RR) were derived through a random-effect model. Differences in primary (biochemical failure, BF; cancer-specific survival, CSS), and secondary outcomes (overall survival, OS; local or distant recurrence, LR/DM) were explored. Absolute differences (AD) and the number needed to treat (NNT) were calculated. Heterogeneity, a meta-regression for clinic-pathological predictors and a correlation test for surrogates were conducted.
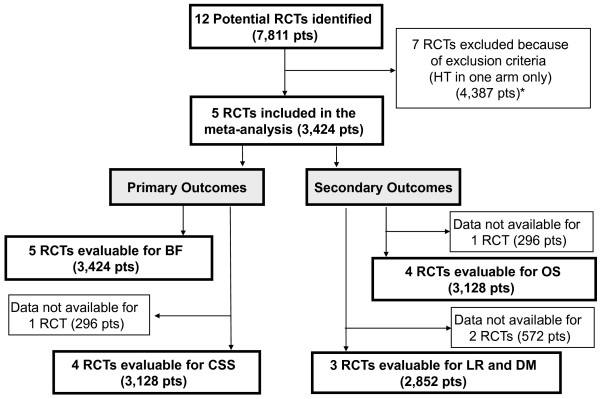
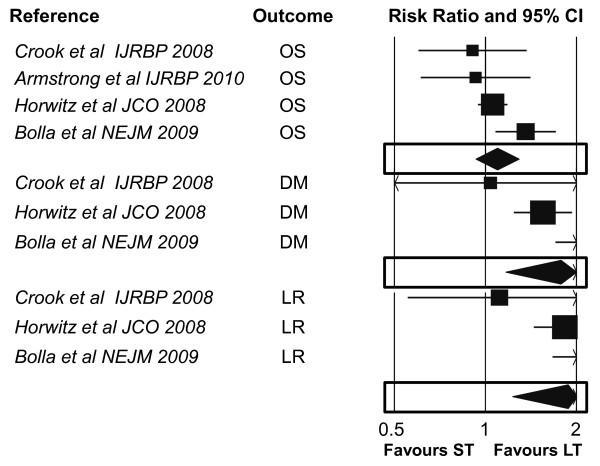
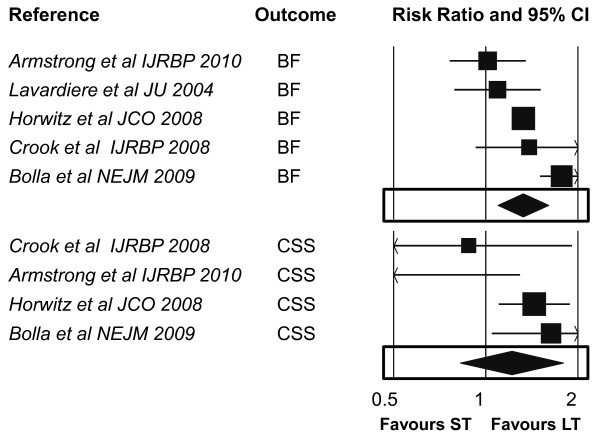
Five trials (3,424 patients) were included. Patient population ranged from 267 to 1,521 patients. The longer hormonal treatment significantly improves BF (with significant heterogeneity) with an absolute benefit of 10.1%, and a non significant trend in CSS. With regard to secondary end-points, the longer hormonal treatment significantly decrease both the LR and the DM with an absolute difference of 11.7% and 11.5%. Any significant difference in OS was observed. None of the three identified clinico-pathological predictors (median PSA, range 9.5-20.35, Gleason score 7-10, 27-55% patients/trial, and T3-4, 13-77% patients/trial), did significantly affect outcomes. At the meta-regression analysis a significant correlation between the overall treatment benefit in BF, CSS, OS, LR and DM, and the length of the treatment was found (p ≤ 0.03).
Although with significant heterogeneity (reflecting different patient' risk stratifications), a longer hormonal treatment duration significantly decreases biochemical, local and distant recurrences, with a trend for longer cancer specific survival.
激素治疗联合放疗显著降低局部晚期前列腺癌患者的复发率和死亡率。为了确定激素治疗持续时间是否存在差异,进行了基于文献的荟萃分析。
通过随机效应模型得出相对风险(RR)。探讨了主要结局(生化失败,BF;癌症特异性生存,CSS)和次要结局(总生存,OS;局部或远处复发,LR/DM)的差异。计算绝对差异(AD)和需要治疗的人数(NNT)。进行了异质性、临床病理预测因素的荟萃回归分析和替代指标的相关性检验。
纳入了五项试验(3424 名患者)。患者人群范围从 267 到 1521 名患者。较长的激素治疗显著改善 BF(具有显著异质性),绝对获益为 10.1%,CSS 呈非显著趋势。关于次要终点,较长的激素治疗显著降低 LR 和 DM,绝对差异分别为 11.7%和 11.5%。OS 没有观察到任何显著差异。三个确定的临床病理预测因素(中位 PSA,范围 9.5-20.35,Gleason 评分 7-10,27-55%的患者/试验,和 T3-4,13-77%的患者/试验)均未显著影响结局。在荟萃回归分析中,BF、CSS、OS、LR 和 DM 的总体治疗获益与治疗持续时间之间存在显著相关性(p≤0.03)。
尽管存在显著的异质性(反映了不同患者的风险分层),但较长的激素治疗持续时间可显著降低生化、局部和远处复发的风险,同时 CSS 也有延长的趋势。