Renal-Electrolyte Division, University of Pittsburgh, Pittsburgh, USA.
BMC Nephrol. 2011 Mar 15;12:12. doi: 10.1186/1471-2369-12-12.
Chronic kidney disease (CKD) is a common disorder associated with increased morbidity and mortality. Primary care physicians (PCPs) care for the majority of pre-dialysis CKD patients; however, PCPs often do not recognize the presence of CKD based on serum creatinine levels. Prior studies suggest that PCPs and nephrologists deliver suboptimal CKD care. One strategy to improve disease awareness and treatment is estimated glomerular filtration rate (eGFR) reporting. We examined PCP and nephrologist CKD practices before and after routine eGFR reporting.
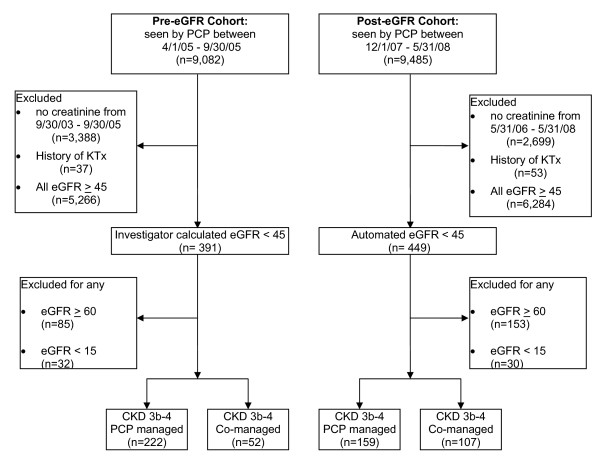
We conducted a retrospective cohort study of patients with CKD 3b-4 (eGFR < 45) seen at a university-based, outpatient primary care clinic. Using a chi-square or Fisher's exact test, we compared co-management rates, renal protective strategies, CKD documentation, and laboratory processes of care in 274 patients and 266 patients seen in a 6-month period prior to and following eGFR implementation, respectively.
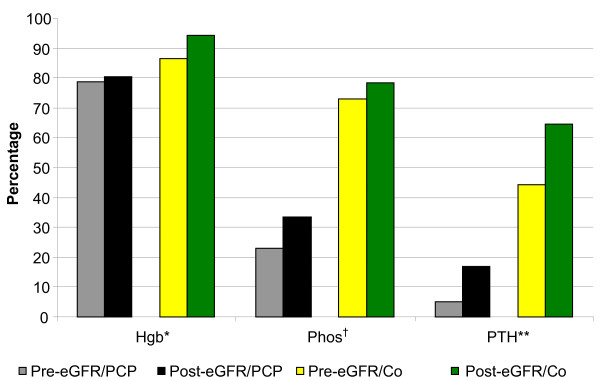
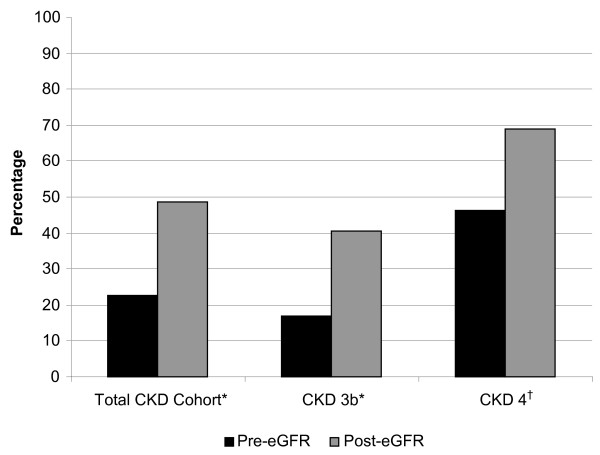
CKD co-management increased from 22.6% pre-eGFR to 48.5% post-eGFR (P < 0.0001). eGFR reporting did not improve angiotensin converting enzyme inhibitor or angiotensin receptor blocker use or quantitative urinary testing. However, non-steroidal anti-inflammatory drug avoidance (pre-eGFR 81.8% vs. post- eGFR 90.6%, P = 0.003) and phosphorus and parathyroid hormone testing improved (pre-eGFR vs. post-eGFR: 32.5% vs. 51.5%, P < 0.0001; 12.4% vs. 36.1%, P < 0.0001 respectively).
A marked increase in CKD co-management was observed following eGFR implementation. Although some improvements in processes of care were noted, this did not include angiotensin converting enzyme inhibitor or angiotensin receptor blocker use. Overall care remained suboptimal despite eGFR reporting; further strategies are needed to improve PCP and nephrologist CKD care.
慢性肾脏病(CKD)是一种常见的疾病,与发病率和死亡率的增加有关。初级保健医生(PCP)照顾大多数透析前 CKD 患者;然而,PCP 通常无法根据血清肌酐水平识别 CKD 的存在。先前的研究表明,PCP 和肾病学家提供的 CKD 护理并不理想。提高疾病意识和治疗的一种策略是估计肾小球滤过率(eGFR)报告。我们研究了在常规 eGFR 报告前后 PCP 和肾病学家的 CKD 实践。
我们对在一所大学门诊初级保健诊所就诊的 CKD 3b-4 患者(eGFR <45)进行了回顾性队列研究。使用卡方或 Fisher 精确检验,我们比较了在 eGFR 实施前后 6 个月分别就诊的 274 名和 266 名患者的共同管理率、肾脏保护策略、CKD 记录和实验室护理流程。
CKD 共同管理从 eGFR 前的 22.6%增加到 eGFR 后的 48.5%(P <0.0001)。eGFR 报告并没有改善血管紧张素转换酶抑制剂或血管紧张素受体阻滞剂的使用或定量尿检测。然而,非甾体抗炎药的避免(eGFR 前 81.8%比 eGFR 后 90.6%,P = 0.003)和磷和甲状旁腺激素检测的改善(eGFR 前 32.5%比 eGFR 后 51.5%,P <0.0001;eGFR 前 12.4%比 eGFR 后 36.1%,P <0.0001)。
在实施 eGFR 后,CKD 的共同管理显著增加。尽管注意到一些护理流程的改进,但这并不包括血管紧张素转换酶抑制剂或血管紧张素受体阻滞剂的使用。尽管进行了 eGFR 报告,但整体护理仍然不理想;需要进一步的策略来改善 PCP 和肾病学家的 CKD 护理。