Department of Radiology, Memorial Sloan-Kettering Cancer Center, New York, NY 10065, USA; Department of Radiology, Division of General and Pediatric Radiology, Medical University Vienna, Vienna General Hospital, 1090 Wien, Austria.
Department of Radiology, Memorial Sloan-Kettering Cancer Center, New York, NY 10065, USA.
J Pediatr Surg. 2011 Apr;46(4):729-735. doi: 10.1016/j.jpedsurg.2010.11.027.
To determine if selected computed tomography (CT) characteristics of pulmonary nodules in pediatric patients with osteosarcoma can help distinguish the nodules as benign or malignant.
The institutional review board approved this HIPAA (Health Insurance Portability and Accountability Act-compliant, retrospective study of 30 pediatric osteosarcoma patients (median age 14 years, range 8-22) who underwent chest CT with resection of 117 pulmonary nodules from January 2001 to December 2006. Two pediatric radiologists and one chest radiologist independently and retrospectively reviewed the CT scans and classified nodules as benign, malignant, or indeterminate on the basis of nodule size, laterality, number, location, growth, density, margin appearance, and calcification. Generalized estimating equations were used to examine which characteristics were independent predictors of nodule malignancy.
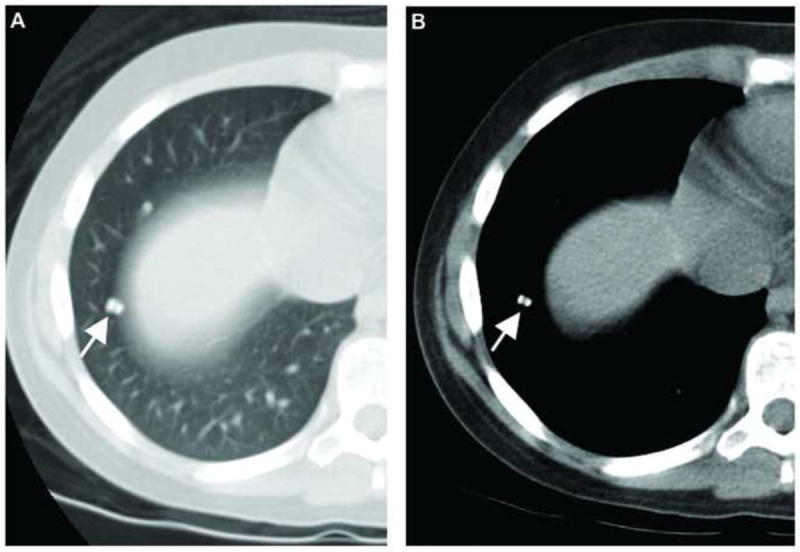
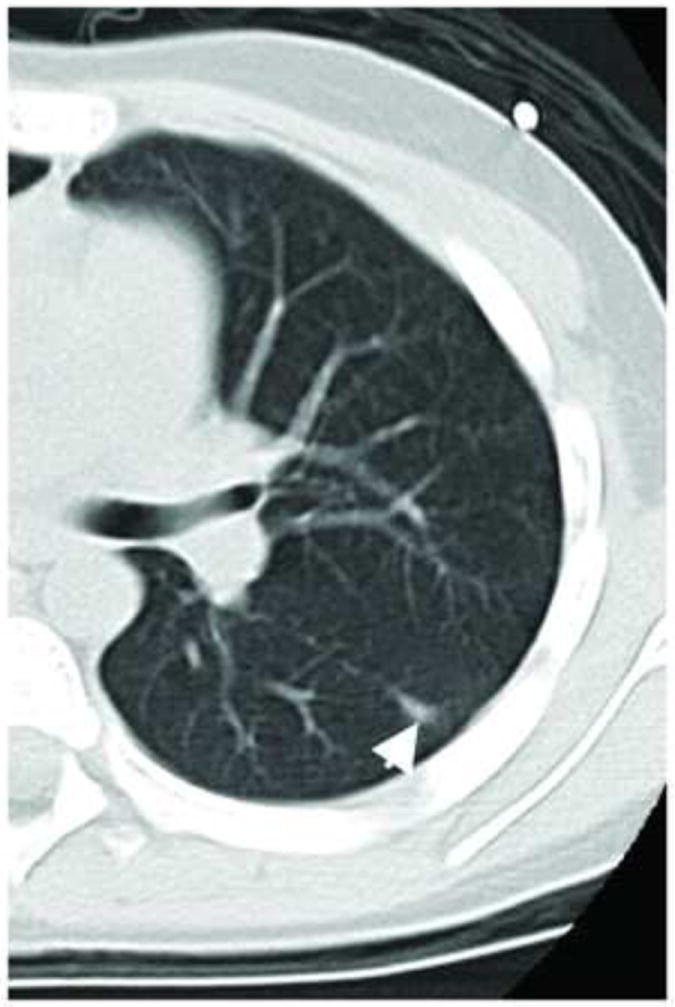
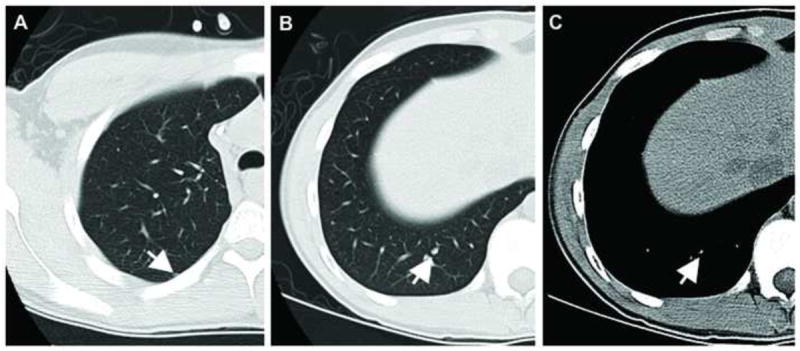
Of the 117 nodules, 80 (68%) were malignant and 37 (32%) were benign by pathologic review. The readers correctly classified 93% to 94% of the malignant nodules. For benign lesions, the results were not as accurate, with the readers correctly classifying only 11% to 30% of lesions. Most of the benign lesions were classified as indeterminate by the readers (54%-65%). Nodule size (≥5 mm) and the presence of calcifications were associated with an increased probability of malignancy (P b .05).
On chest CT, nodule size 5 mm or greater and the presence of calcifications are associated with an increased probability of malignant nodule histology in pediatric patients with osteosarcoma. However, nodule characteristics, apart from size and calcification, at chest CT cannot reliably distinguish benign from malignant pulmonary nodules in these patients.
确定小儿骨肉瘤患者肺部结节的 CT 特征是否有助于区分良恶性。
该机构审查委员会批准了这项 HIPAA(符合健康保险携带和责任法案)合规、回顾性研究,共纳入 30 名小儿骨肉瘤患者(中位年龄 14 岁,范围 8-22 岁),他们于 2001 年 1 月至 2006 年 12 月期间接受胸部 CT 检查并切除了 117 个肺部结节。两名儿科放射科医生和一名胸部放射科医生独立且回顾性地对 CT 扫描进行了评估,并根据结节大小、侧别、数量、位置、生长、密度、边缘外观和钙化情况将结节分为良性、恶性或不确定。广义估计方程用于检查哪些特征是结节恶性的独立预测因素。
117 个结节中,病理检查 80 个(68%)为恶性,37 个(32%)为良性。读者正确分类了 93%-94%的恶性结节。对于良性病变,结果并不准确,读者仅正确分类了 11%-30%的病变。大多数良性病变被读者归类为不确定(54%-65%)。结节大小(≥5mm)和钙化的存在与恶性的可能性增加相关(P b.05)。
在胸部 CT 上,结节大小为 5mm 或更大且存在钙化与小儿骨肉瘤患者恶性结节组织学的可能性增加相关。然而,除了大小和钙化外,这些患者胸部 CT 上的结节特征不能可靠地区分良性和恶性肺部结节。