Department of Pathology, University Medical Center Utrecht, Heidelberglaan 100, PO Box 85500, 3508 GA, Utrecht, The Netherlands.
Cell Oncol (Dordr). 2011 Oct;34(5):475-82. doi: 10.1007/s13402-011-0043-7. Epub 2011 May 6.
Ductal carcinoma in situ (DCIS) accounts for approximately 20% of mammographically detected breast cancers. Although DCIS is generally highly curable, some women with DCIS will develop life-threatening invasive breast cancer, but the determinants of progression to infiltrating ductal cancer (IDC) are largely unknown.
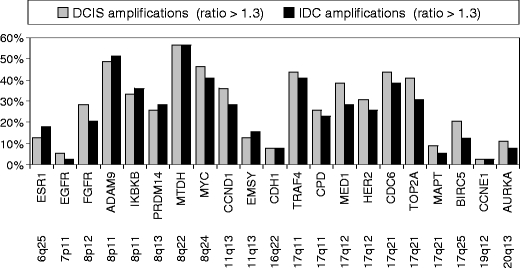
In the current study, we used multiplex ligation-dependent probe amplification (MLPA), a multiplex PCR-based test, to compare copy numbers of 21 breast cancer related genes between laser-microdissected DCIS and adjacent IDC lesions in 39 patients. Genes included in this study were ESR1, EGFR, FGFR1, ADAM9, IKBKB, PRDM14, MTDH, MYC, CCND1, EMSY, CDH1, TRAF4, CPD, MED1, HER2, CDC6, TOP2A, MAPT, BIRC5, CCNE1 and AURKA.
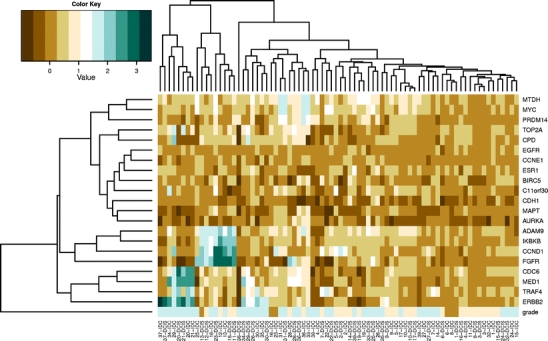
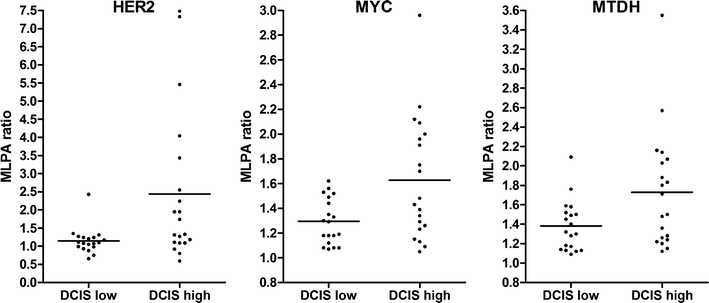
There were no significant differences in copy number for the 21 genes between DCIS and adjacent IDC. Low/intermediate-grade DCIS showed on average 6 gains/amplifications versus 8 in high-grade DCIS (p = 0.158). Furthermore, alterations of AURKA and CCNE1 were exclusively found in high-grade DCIS, and HER2, PRDM14 and EMSY amplification was more frequent in high-grade DCIS than in low/intermediate-grade DCIS. In contrast, the average number of alterations in low/intermediate and high grade IDC was similar, and although EGFR alterations were exclusively found in high grade IDC compared to low/intermediate-grade IDC, there were generally fewer differences between low/intermediate-grade and high-grade IDC than between low/intermediate-grade and high-grade DCIS.
In conclusion, there were no significant differences in copy number for 21 breast cancer related genes between DCIS and adjacent IDC, indicating that DCIS is genetically as advanced as its invasive counterpart. However, high grade DCIS showed more copy number changes than low/intermediate grade DCIS with specifically involved genes, supporting a model in which different histological grades of DCIS are associated with distinct genomic changes that progress to IDC in different routes. These high grade DCIS specific genes may be potential targets for treatment and/or predict progression.
导管原位癌(DCIS)约占乳腺 X 线摄影检测到的乳腺癌的 20%。虽然 DCIS 通常可以治愈,但一些患有 DCIS 的女性会患上危及生命的浸润性乳腺癌,但进展为浸润性导管癌(IDC)的决定因素在很大程度上尚不清楚。
在本研究中,我们使用多重连接依赖性探针扩增(MLPA),一种基于多重 PCR 的测试,比较了 39 例患者中激光微切割 DCIS 和相邻 IDC 病变的 21 个乳腺癌相关基因的拷贝数。本研究中包含的基因有 ESR1、EGFR、FGFR1、ADAM9、IKBKB、PRDM14、MTDH、MYC、CCND1、EMSY、CDH1、TRAF4、CCPD、MED1、HER2、CDC6、TOP2A、MAPT、BIRC5、CCNE1 和 AURKA。
DCIS 和相邻 IDC 之间 21 个基因的拷贝数没有显著差异。低/中等级 DCIS 平均有 6 次增益/扩增,而高等级 DCIS 有 8 次(p=0.158)。此外,AURKA 和 CCNE1 的改变仅在高等级 DCIS 中发现,而 HER2、PRDM14 和 EMSY 的扩增在高等级 DCIS 中比低/中等级 DCIS 更频繁。相反,低/中等级和高等级 IDC 的平均改变数量相似,虽然 EGFR 的改变仅在高等级 IDC 中发现,而在低/中等级 IDC 中未发现,但低/中等级 IDC 和高等级 IDC 之间的差异一般比低/中等级 DCIS 和高等级 DCIS 之间的差异小。
总之,DCIS 和相邻 IDC 之间 21 个乳腺癌相关基因的拷贝数没有显著差异,表明 DCIS 在遗传上与浸润性癌相当。然而,高等级 DCIS 比低/中等级 DCIS 显示出更多的拷贝数变化,涉及特定的基因,支持这样一种模型,即不同组织学等级的 DCIS 与不同的基因组变化相关,这些变化以不同的途径进展为 IDC。这些高等级 DCIS 特定的基因可能是治疗的潜在靶点和/或预测进展的指标。