Bhaskar Emmanuel, Kumar Bismay, Ramalakshmi S
Department of Medicine, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, India.
Indian J Crit Care Med. 2010 Oct;14(4):170-4. doi: 10.4103/0972-5229.76079.
Acute symptomatic hyponatremia is a frequent yet poorly studied clinical problem.
To develop a non-weight based protocol for the treatment of acute symptomatic hyponatremia.
Observational study in a Multi-disciplinary Intensive Care Unit of an urban tertiary care hospital.
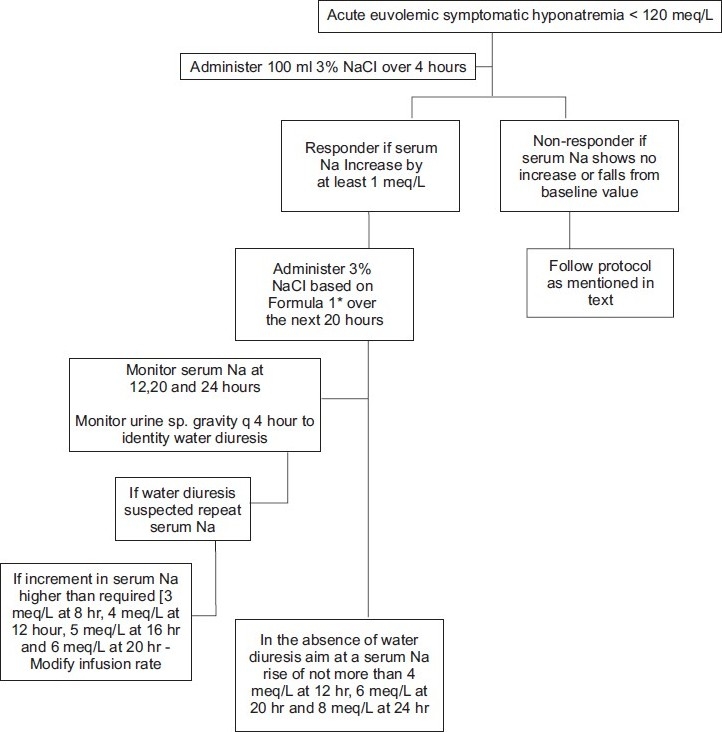
Patients aged >18 years, admitted with euvolemic acute symptomatic severe hyponatremia (defined as serum sodium <120 meq/l with symptoms <24 hours), formed the study population. On confirmation of euvolemic status clinically and by laboratory investigations, patients were administered 100 ml of 3% NaCl over a period of 4 hours irrespective of the weight of the patient, followed by reassessment of serum Na at the end of 4 hours. The volume of hypertonic saline (in ml) required to increase serum Na by 8 meq/l was calculated using the formula: 100 × 8/increment in serum Na observed with 100 ml hypertonic saline. This volume was infused over the next 20 hours. To monitor renal water diuresis which may contribute to overcorrection, the urine specific gravity was monitored every 4 hours for sudden decrease of ≥ 0.010 from the baseline value. Measurement of serum Na was repeated if a fall in the urine specific gravity was observed and subsequently repeated every 4 hours. If no fall occurs in urine specific gravity, serum Na measurement was repeated at 12, 20 and at 24 hours (0 hour being the initiation of 100 ml hypertonic saline). The volume of infusate was adjusted if an excessive increment of serum Na (greater than 3 meq at 8 hours, 4 meq at 12 hours, 5 meq at 16 hours and 6 meq at 20 hours) was observed. Baseline characteristics were compared using chi-square test and Mann-Whitney U test.
58 patients formed the study cohort. The mean age was 58 years. The mean serum Na on admission was 114 meq/l. Administration of 100 ml hypertonic saline resulted in a mean increase in serum Na of 2 meq/l. The mean increase in serum Na over 24 hours was 9 meq/l and mean volume of hypertonic saline required for a serum Na increment of 8 meq/l was 600 ml.
The non-weight based protocol with monitoring for water diuresis is reasonably an effective strategy in the treatment of acute euvolemic symptomatic hyponatremia.
急性症状性低钠血症是一个常见但研究较少的临床问题。
制定一种基于非体重的急性症状性低钠血症治疗方案。
在一家城市三级护理医院的多学科重症监护病房进行的观察性研究。
年龄>18岁、因等容性急性症状性严重低钠血症(定义为血清钠<120 meq/l且症状持续时间<24小时)入院的患者构成研究人群。经临床和实验室检查确认等容状态后,无论患者体重如何,均在4小时内给予100 ml 3%氯化钠,然后在4小时结束时重新评估血清钠。使用公式计算使血清钠升高8 meq/l所需的高渗盐水体积(以ml为单位):100×8/100 ml高渗盐水观察到的血清钠增加值。该体积在接下来的20小时内输注。为监测可能导致过度纠正的肾性水利尿,每4小时监测尿比重,观察其是否从基线值突然下降≥0.010。如果观察到尿比重下降,则重复测量血清钠,随后每4小时重复一次。如果尿比重未下降,则在12、20和24小时(0小时为开始输注100 ml高渗盐水的时间)重复测量血清钠。如果观察到血清钠过度升高(8小时时大于3 meq,12小时时大于4 meq,16小时时大于5 meq,20小时时大于6 meq),则调整输注液体积。使用卡方检验和曼-惠特尼U检验比较基线特征。
58名患者构成研究队列。平均年龄为58岁。入院时平均血清钠为114 meq/l。给予100 ml高渗盐水后,血清钠平均升高2 meq/l。24小时内血清钠平均升高9 meq/l,使血清钠升高8 meq/l所需的高渗盐水平均体积为600 ml。
基于非体重的方案并监测水利尿在治疗急性等容性症状性低钠血症方面是一种相当有效的策略。