Department of Gastroenterology and Hepatology, Erasmus Medical Centre, Room Ba393, PO Box 2040, 3000 CA Rotterdam, The Netherlands.
Br J Cancer. 2011 Jul 12;105(2):200-5. doi: 10.1038/bjc.2011.214. Epub 2011 Jun 14.
The interval between the onset of Barrett's oesophagus (BO) and oesophageal adenocarcinoma (OAC) can be termed the incubation period. However, the unrecorded onset of BO precludes its direct observation.
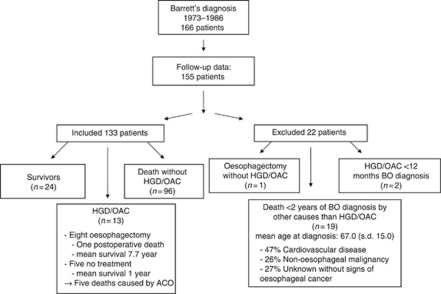
Determining the range of intervals between BO diagnosis and OAC within the longest observational BO follow-up study. Exclusion criteria were presence of high-grade dysplasia (HGD) or OAC at baseline, death within <2 years of BO diagnosis, oesophagectomy without HGD/OAC and loss to follow-up. A total of 133 patients (M/F 73/60) were taken into account.
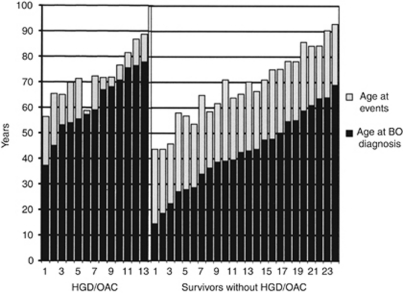
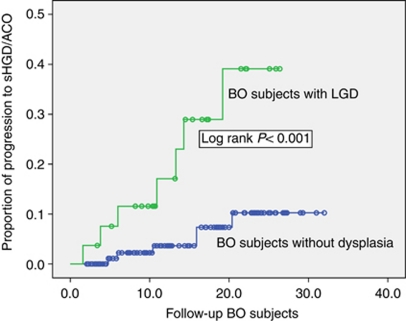
In 1967 person years of follow-up there were 13 cases of HGD/OAC, (0.66% p.a.; 95% CI 0.58-0.74), 96 patients died without HGD/OAC and 24 survived without HGD/OAC. The mean intervals between BO diagnosis and either HGD/OAC, death or end of follow-up were 10.8, 12.6 and 25.5 years, respectively, and the mean ages at endpoint were 72.5, 80.0 and 68.3 years, respectively. The survivors without HGD/OAC had a lower age at BO diagnosis (mean 42.8 vs 61.2 and 67.4 years, P<0.001). Baseline presence of low-grade dysplasia was associated with progression to HGD/OAC (log rank P<0.001).
The Rotterdam BO follow-up cohort revealed a long incubation period between onset of BO and development of HGD/OAC, in patients without HGD/OAC at baseline as illustrated by 24 patients diagnosed with BO at a young age and followed for a mean period of 25.5 years. Their tumour-free survival established a minimum incubation period, suggesting a true incubation period of three decades or more.
巴雷特食管(BO)和食管腺癌(OAC)之间的间隔时间可称为潜伏期。然而,BO 的无记录发病使其无法直接观察。
确定最长 BO 随访研究中 BO 诊断与 OAC 之间的间隔范围。排除标准为基线时存在高级别异型增生(HGD)或 OAC、BO 诊断后 2 年内死亡、无 HGD/OAC 的食管切除术以及失访。共纳入 133 例患者(M/F 73/60)。
在 1967 人年的随访中,有 13 例 HGD/OAC(0.66%p.a.;95%CI0.58-0.74),96 例患者无 HGD/OAC 死亡,24 例无 HGD/OAC 存活。BO 诊断与 HGD/OAC、死亡或随访结束之间的平均间隔分别为 10.8、12.6 和 25.5 年,终点年龄分别为 72.5、80.0 和 68.3 岁。无 HGD/OAC 的幸存者 BO 诊断年龄较低(分别为 42.8、61.2 和 67.4 岁,P<0.001)。基线存在低级别异型增生与进展为 HGD/OAC 相关(对数秩 P<0.001)。
鹿特丹 BO 随访队列显示,在基线时无 HGD/OAC 的患者中,BO 发病与 HGD/OAC 发展之间存在较长的潜伏期,如图中 24 例 BO 诊断年龄较小的患者所示,随访时间平均为 25.5 年。他们的无肿瘤生存确立了最短的潜伏期,提示潜伏期真实存在三十年或更长时间。