Intensive Care Unit, Section Thorax-Vascular Disease-Abdomen-Metabolism, Ambroise Paré University Hospital, AP-HP, 9 Av Charles de Gaulle, F-92104 Boulogne-Billancourt Cedex, France.
Crit Care. 2011 Jul 25;15(4):R175. doi: 10.1186/cc10324.
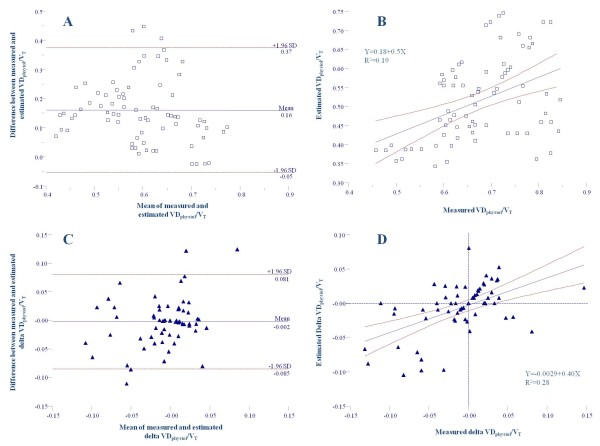
Our aims in this study were to report changes in the ratio of alveolar dead space to tidal volume (VDalv/VT) in the prone position (PP) and to test whether changes in partial pressure of arterial CO2 (PaCO2) may be more relevant than changes in the ratio of partial pressure of arterial O2 to fraction of inspired O2 (PaO2/FiO2) in defining the respiratory response to PP. We also aimed to validate a recently proposed method of estimation of the physiological dead space (VDphysiol/VT) without measurement of expired CO2.
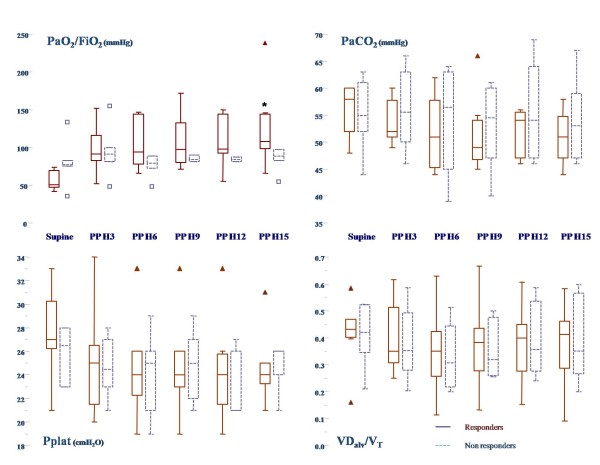
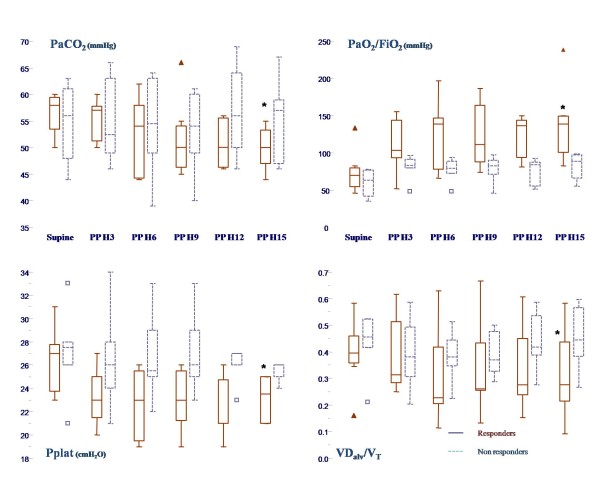
Thirteen patients with a PaO2/FiO2 ratio < 100 mmHg were included in the study. Plateau pressure (Pplat), positive end-expiratory pressure (PEEP), blood gas analysis and expiratory CO2 were recorded with patients in the supine position and after 3, 6, 9, 12 and 15 hours in the PP. Responders to PP were defined after 15 hours of PP either by an increase in PaO2/FiO2 ratio > 20 mmHg or by a decrease in PaCO2 > 2 mmHg. Estimated and measured VDphysiol/VT ratios were compared.
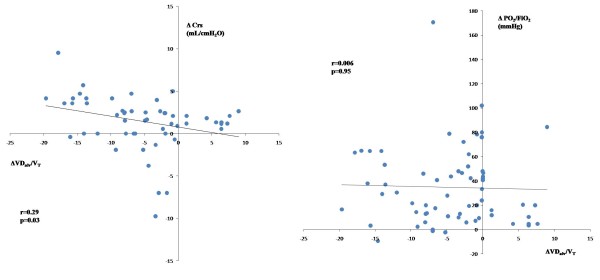
PP induced a decrease in Pplat, PaCO2 and VDalv/VT ratio and increases in PaO2/FiO2 ratios and compliance of the respiratory system (Crs). Maximal changes were observed after six to nine hours. Changes in VDalv/VT were correlated with changes in Crs, but not with changes in PaO2/FiO2 ratios. When the response was defined by PaO2/FiO2 ratio, no significant differences in Pplat, PaCO2 or VDalv/VT alterations between responders (n = 7) and nonresponders (n = 6) were observed. When the response was defined by PaCO2, four patients were differently classified, and responders (n = 7) had a greater decrease in VDalv/VT ratio and in Pplat and a greater increase in PaO2/FiO2 ratio and in Crs than nonresponders (n = 6). Estimated VDphysiol/VT ratios significantly underestimated measured VDphysiol/VT ratios (concordance correlation coefficient 0.19 (interquartile ranges 0.091 to 0.28)), whereas changes during PP were more reliable (concordance correlation coefficient 0.51 (0.32 to 0.66)).
PP induced a decrease in VDalv/VT ratio and an improvement in respiratory mechanics. The respiratory response to PP appeared more relevant when PaCO2 rather than the PaO2/FiO2 ratio was used. Estimated VDphysiol/VT ratios systematically underestimated measured VDphysiol/VT ratios.
本研究旨在报告在俯卧位(PP)时肺泡死腔与潮气量(VDalv/VT)比值的变化,并检验动脉血二氧化碳分压(PaCO2)的变化是否比动脉血氧分压与吸入氧分数比(PaO2/FiO2)比值的变化更能反映对 PP 的呼吸反应。我们还旨在验证一种最近提出的不测量呼气 CO2 即可估算生理死腔(VDphysiol/VT)的方法。
纳入了 13 名 PaO2/FiO2 比值<100mmHg 的患者。在仰卧位和俯卧位 3、6、9、12 和 15 小时时记录平台压(Pplat)、呼气末正压(PEEP)、血气分析和呼气 CO2。15 小时后,如果 PaO2/FiO2 比值增加>20mmHg 或 PaCO2 降低>2mmHg,则将患者定义为对 PP 有反应。比较了估计的和测量的 VDphysiol/VT 比值。
PP 导致 Pplat、PaCO2 和 VDalv/VT 比值降低,以及动脉血氧分压与吸入氧分数比(PaO2/FiO2)比值和呼吸系统顺应性(Crs)增加。最大变化发生在 6 至 9 小时。VDalv/VT 的变化与 Crs 的变化相关,但与 PaO2/FiO2 比值的变化无关。当以 PaO2/FiO2 比值来定义反应时,对反应者(n=7)和无反应者(n=6)之间的 Pplat、PaCO2 或 VDalv/VT 变化没有观察到显著差异。当以 PaCO2 来定义反应时,4 名患者被不同分类,反应者(n=7)的 VDalv/VT 比值、Pplat 降低更明显,而 PaO2/FiO2 比值和 Crs 增加更明显,与无反应者(n=6)相比。估计的 VDphysiol/VT 比值显著低估了测量的 VDphysiol/VT 比值(一致性相关系数 0.19(四分位间距 0.091 至 0.28)),而在 PP 期间的变化则更可靠(一致性相关系数 0.51(0.32 至 0.66))。
PP 导致 VDalv/VT 比值降低和呼吸力学改善。当使用 PaCO2 而不是 PaO2/FiO2 比值来定义对 PP 的反应时,呼吸反应似乎更相关。估计的 VDphysiol/VT 比值系统地低估了测量的 VDphysiol/VT 比值。