Department of Medicine and Comprehensive Cancer Center, University of Chicago, Chicago IL, USA.
Mediterr J Hematol Infect Dis. 2011;3(1):e2011032. doi: 10.4084/MJHID.2011.032. Epub 2011 Jul 8.
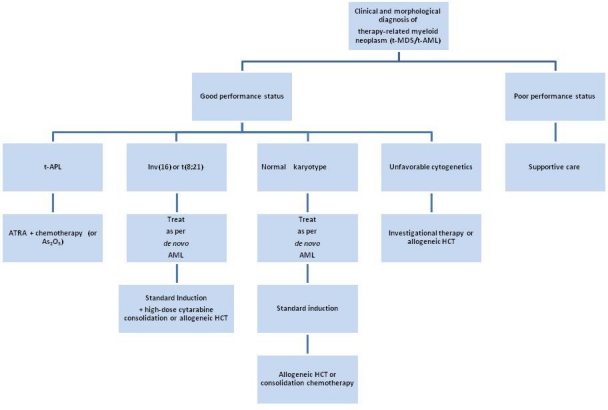
Treatment for a pre-existing condition using chemotherapy, radiation therapy, immunosuppressive therapy, or a combination of these modalities may lead to the devastating complication of therapy-related myelodysplastic syndrome or acute myeloid leukemia (t-MDS/t-AML), collectively known as therapy-related myeloid neoplasm (t-MN). This disorder arises as a direct consequence of mutational events induced by the primary treatment. The outcomes for these patients have been historically poor compared to people who develop AML de novo. Currently comprising 10-20% of all cases of AML, t-MN is relatively resistant to conventional leukemia therapies, and is associated with s ort survival times. Median life expectancy from diagnosis is about 8-10 months in most series. Although the spectrum of cytogenetic abnormalities in t-AML is similar to AML de novo, the frequency of unfavorable cytogenetics, such as a complex karyotype or deletion or loss of chromosomes 5 and/or 7, is considerably higher in t-MN. Two distinct groups of patients with t-MN have been described. The more common subtype, seen in about 75% of patients, typically occurs 5-7 years after first exposure to alkylating agents or radiation, is often preceded by a myelodysplastic syndrome (MDS), and is frequently accompanied by clonal cytogenetic abnormalities such as the loss of all or part of chromosomes 5 or 7. Mutations of the P53 tumor suppressor gene are also common. The risk is related to total cumulative exposure over time to alkylating agents. In contrast, among individuals who develop t-AML after treatment with topoisomerase II inhibitors, the latency period to the development of t-AML is often only 1-3 years, antecedent MDS is rare, and gene rearrangements involving MLL at 11q23 or RUNX1/AML1 at 21q22 are common. It is now well recognized that APL and other subtypes of AML with balanced translocations sometimes occur as therapy-related myeloid neoplasms (t-MN) in patients who have previously received cytotoxic therapy or ionizing radiation therapy (RT). The most of this review will focus on these "good risk" leukemias, i.e. those with APL or inv(16)/t(16;16) or t(8;21).
使用化疗、放疗、免疫抑制疗法或这些方法的组合治疗先前存在的疾病可能会导致灾难性的治疗相关骨髓增生异常综合征或急性髓系白血病(t-MDS/t-AML)并发症,统称为治疗相关髓系肿瘤(t-MN)。这种疾病是原发性治疗引起的突变事件的直接后果。与新发 AML 患者相比,这些患者的预后一直较差。目前,t-MN 约占所有 AML 病例的 10-20%,相对抵抗常规白血病治疗,且生存时间较短。在大多数系列中,从诊断到中位预期寿命约为 8-10 个月。尽管 t-AML 的细胞遗传学异常谱与新发 AML 相似,但在 t-MN 中,不良细胞遗传学的频率相当高,如复杂核型或 5 号和/或 7 号染色体缺失或丢失。已经描述了 t-MN 的两种不同患者群体。更常见的亚型,见于约 75%的患者,通常在首次接触烷化剂或放疗后 5-7 年内发生,常伴有骨髓增生异常综合征(MDS),常伴有克隆细胞遗传学异常,如 5 号或 7 号染色体全部或部分缺失。P53 肿瘤抑制基因的突变也很常见。风险与随着时间的推移总累积暴露于烷化剂有关。相比之下,在接受拓扑异构酶 II 抑制剂治疗后发生 t-AML 的个体中,发展为 t-AML 的潜伏期通常仅为 1-3 年,前驱 MDS 罕见,涉及 11q23 处 MLL 或 21q22 处 RUNX1/AML1 的基因重排很常见。现在已经认识到,先前接受细胞毒性治疗或电离辐射治疗(RT)的患者中,有时会出现平衡易位的 APL 和其他 AML 亚型作为治疗相关髓系肿瘤(t-MN)。本综述的重点将放在这些“低危”白血病上,即具有 APL 或 inv(16)/t(16;16)或 t(8;21)的白血病。