Singh Jaswinder, Jain Karun, Ravishankar R
Department of Orthopaedics, JSS Medical College, Mysore, India.
Indian J Orthop. 2011 Sep;45(5):432-8. doi: 10.4103/0019-5413.83764.
The proximal phalanx (PP) of the fingers is fractured more frequently than the middle or even distal phalanges. The problems of malunion, stiffness and sometimes loss of skin or other soft tissues associated with PP fracture increases the disability. The optimum treatment depends on fracture location, fracture geometry and fracture stability. The objective of the study was to analyse the treatment outcome in a series of closed proximal phalangeal fractures of the hand.
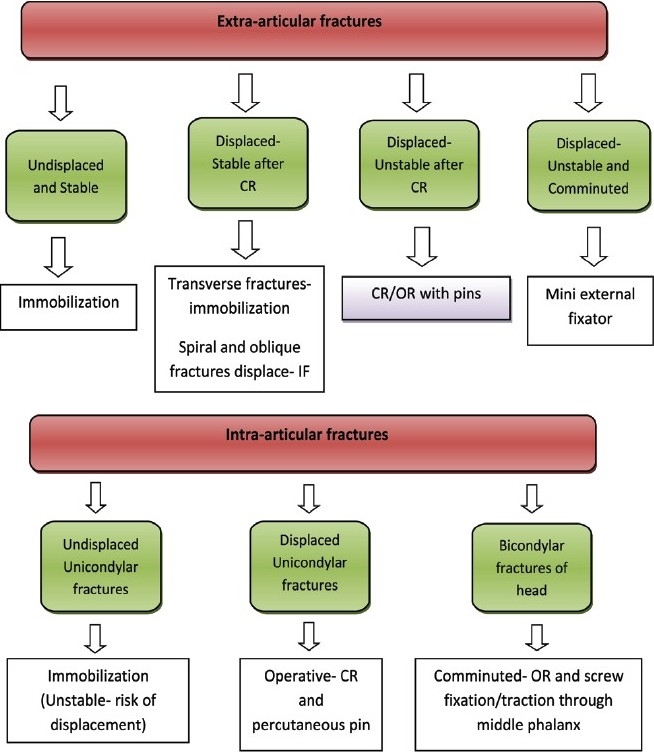
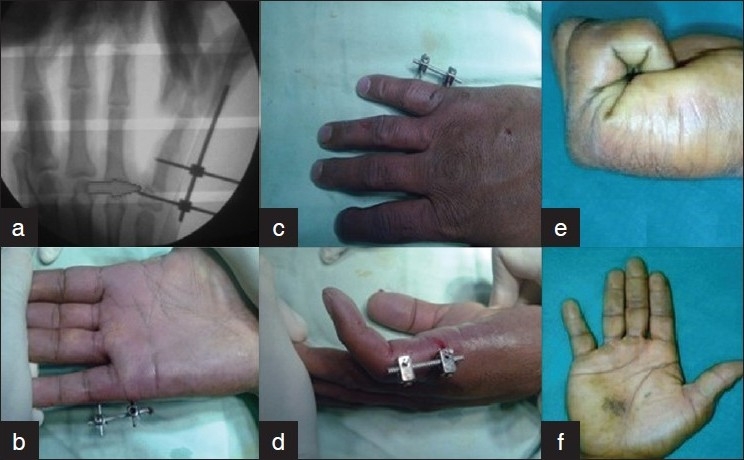
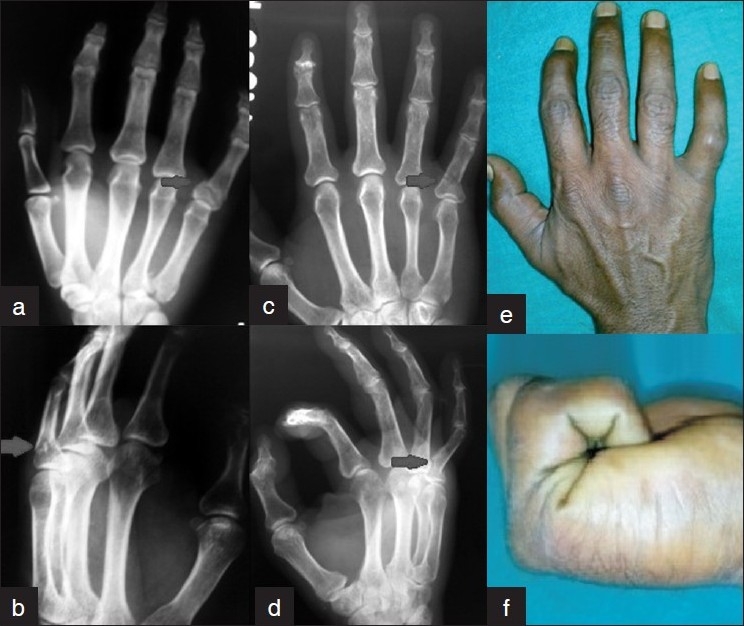
Eighty-four proximal phalangeal fractures in 68 patients were enrolled from 2007 to 2009. The treatment modalities were broadly categorised into two groups, Group A consisted of conservative treatment, and Group B consisted of surgical treatment. Group A included 47 digits treated with closed reduction (CR) with immobilization (n=43), extension block cast and dynamic traction (n=4), while 37 digits were treated in Group B, which included closed or open reduction (OR) and internal fixation (IF) with K-wires (n=31), OR and IF with stainless-steel wiring (n=2), and mini external-fixator (n=4). Belsky's criteria and Gingrass' criteria were used for assessment of finger injuries and to assess the efficacy of conservative and surgical modalities for closed proximal phalangeal fractures of the hand.
Average period of follow-up was 1 year (range 10-14 months). The excellent to good results seen in Groups A and B were 89% and 92%, respectively. Six complications were seen in Group A, which included four cases with malunion and two cases with digital stiffness. Three complications were seen in Group B, which included one each of malunion, digital stiffness and extensor lag. Overall, maximum poor results (n=4) were seen with CR and buddy strapping.
Conservative treatment is an inexpensive method, particularly suitable for stable fractures, and in patients who are poor candidates for surgery, Surgical modalities have distinct advantage of stable fixation, but with added risk of digital stiffness. Percutaneous pinning is a reliable, most commonly used surgical modality and technically easier. Both conservative and surgical modalities have good efficacy when used judiciously.
手指近节指骨(PP)骨折比中节指骨甚至远节指骨骨折更为常见。PP骨折相关的畸形愈合、僵硬以及有时出现的皮肤或其他软组织缺失问题会增加残疾程度。最佳治疗方法取决于骨折部位、骨折形态和骨折稳定性。本研究的目的是分析一系列手部闭合性近节指骨骨折的治疗结果。
2007年至2009年纳入68例患者的84例近节指骨骨折。治疗方式大致分为两组,A组为保守治疗,B组为手术治疗。A组包括47指采用闭合复位(CR)加固定(n = 43)、伸展阻滞石膏固定和动态牵引(n = 4)治疗,而B组37指接受治疗,包括闭合或切开复位(OR)并用克氏针内固定(IF)(n = 31)、OR并用不锈钢丝IF(n = 2)以及微型外固定架(n = 4)。采用Belsky标准和Gingrass标准评估手指损伤情况以及评估保守和手术方式治疗手部闭合性近节指骨骨折的疗效。
平均随访时间为1年(范围10 - 14个月)。A组和B组的优良率分别为89%和92%。A组出现6例并发症,包括4例畸形愈合和2例手指僵硬。B组出现了3例并发症,包括畸形愈合、手指僵硬和伸肌滞后各1例。总体而言,CR和搭伴绷带固定的效果最差(n = 4)。
保守治疗是一种成本低廉的方法,特别适用于稳定骨折以及手术条件不佳的患者。手术方式具有稳定固定的明显优势,但存在手指僵硬的额外风险。经皮穿针固定是一种可靠且最常用的手术方式,技术上也更容易。保守和手术方式在合理应用时均具有良好疗效。