Choto Regis, Chadambuka Addmore, Shambira Gerald, Gombe Notion, Tshimanga Mufuta, Midzi Stanley, Mberikunashe Joseph
MPH Programme, Department of Community Medicine, University of Zimbabwe, Zimbabwe.
Pan Afr Med J. 2012;11:2. Epub 2012 Jan 11.
Since adoption of the measles case-based surveillance system in Zimbabwe in 1998, data has been routinely collected at all levels of the health delivery system and sent to national level with little or no documented evidence of use to identify risky populations, monitor impact of interventions and measure progress towards achieving measles elimination. We analysed this data to determine trends in the national measles case-based surveillance system (NMCBSS).
A retrospective record review of the NMCBSS dataset for period 1999 -2008 was conducted, assessing trends in proportions of investigated cases; timeliness and nature of specimens received at laboratory; timeliness of feedback of serology results, proportion of cases confirmed as measles and national annualized rates of investigation. Comparisons with WHO performance indicators were done. The secondary data analysis was done in Excel and Epi-Info statistical software.
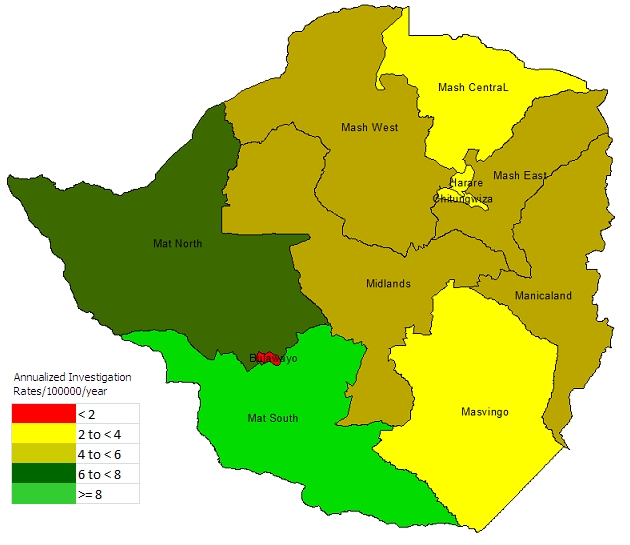
Cumulatively 4994 suspected cases were reported and investigated between 1999 and 2008. Reported suspected and confirmed measles cases declined from 24, 5% and 5.9% respectively in 2000 to 3.9% and 1.0% respectively in 2008. Proportion of cases with blood specimens collected and proportion reaching laboratory timely increased from 83% and 65% respectively in 1999, to 100% and 82% respectively in 2008. Proportion of specimens arriving at laboratory in good condition improved from 65% in 2004 to 94% in 2008 while timeliness of feedback of serology results improved from 4% in 2004 to 65% in 2008. Sensitivity of the NMCBSS however has been weakening, declining from 9.04 cases investigated per 100,000 population per year in 2000 to 1.58 cases/100,000/year in 2008.
The NMCBSS improved in quality, timeliness and feedback of laboratory results of specimens sent for investigation, but its sensitivity declined mainly due to reduced capacity to detect and confirm measles cases. We recommend training staff on active surveillance of cases and more support and supervisory visits to strengthen EPI surveillance.
自1998年津巴布韦采用基于病例的麻疹监测系统以来,卫生服务系统各级定期收集数据并上报至国家层面,但用于识别高危人群、监测干预措施影响以及衡量消除麻疹进展情况的记录证据很少或没有。我们分析了这些数据,以确定国家基于病例的麻疹监测系统(NMCBSS)的趋势。
对1999 - 2008年期间NMCBSS数据集进行回顾性记录审查,评估调查病例比例、实验室收到标本的及时性和性质、血清学结果反馈的及时性、确诊为麻疹的病例比例以及国家年度调查率的趋势。与世界卫生组织的绩效指标进行了比较。二次数据分析在Excel和Epi-Info统计软件中进行。
1999年至2008年期间,累计报告并调查了4994例疑似病例。报告的疑似和确诊麻疹病例分别从2000年的24.5%和5.9%降至2008年的3.9%和1.0%。采集血液标本的病例比例和及时送达实验室的比例分别从1999年的83%和65%增至2008年的100%和82%。送达实验室时状况良好的标本比例从2004年的65%提高到2008年的94%,而血清学结果反馈的及时性从2004年的4%提高到2008年的65%。然而,NMCBSS的敏感性一直在减弱,从2000年每年每10万人口调查9.04例降至2008年的1.58例/10万/年。
NMCBSS在送检标本的实验室结果质量、及时性和反馈方面有所改善,但其敏感性下降主要是由于检测和确诊麻疹病例的能力降低。我们建议对工作人员进行病例主动监测培训,并增加支持和监督访问,以加强扩大免疫规划监测。