Institute for Diagnostic and Interventional Radiology, Johann Wolfgang Goethe-University, Theodor-Stern-Kai 7, 60590 Frankfurt am Main, Germany.
Br J Cancer. 2012 Mar 27;106(7):1274-9. doi: 10.1038/bjc.2012.69. Epub 2012 Mar 1.
To evaluate a treatment protocol with repeated transarterial-chemoembolisation (TACE) downsizing before MR-guided laser-induced interstitial thermotherapy (LITT) using different chemotherapeutic combinations in patients with unresectable colorectal cancer (CRC) liver metastases.
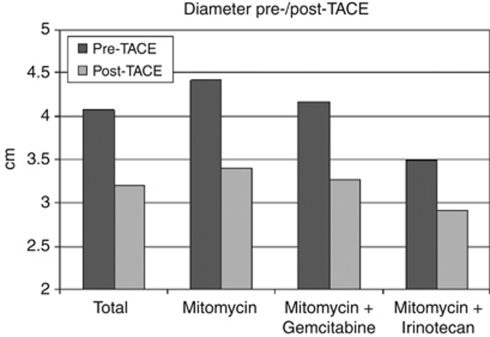
Two hundred and twenty-four patients were included in the current study. Transarterial-chemoembolisation (mean 3.4 sessions per patient) was performed as a downsizing treatment to meet the LITT requirements (number5, diameter <5 cm). The intra-arterial protocol consisted of either Irinotecan and Mitomycin (n=77), Gemcitabine and Mitomycin (n=49) or Mitomycin alone (n=98) in addition to Lipiodol and Embocept in all patients. Post TACE, all patients underwent LITT (mean 2.2 sessions per patient).
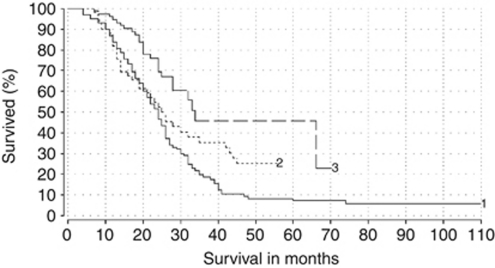
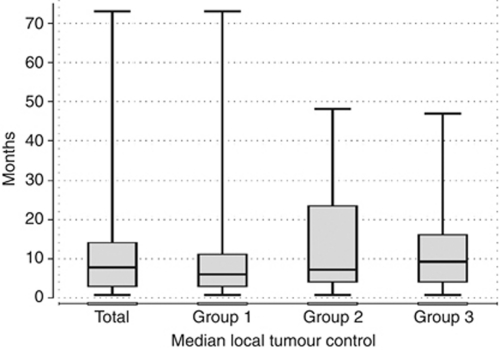
Overall, TACE resulted in a mean reduction in diameter of the target lesions of 21.4%. The median time to progression was 8 months, calculated from the start of therapy and the median local tumour control rate was 7.5 months, calculated as of therapy completion. Median survival of patients calculated from the beginning of TACE was 23 months (range 4-110 months), in patients treated with Irinotecan and Mitomycin the median was 22.5 months, Gemcitabine and Mitomycin 23 months and Mitomycin only 24 months with a statistically significant difference between the groups (P<0.01).
Repeated TACE offers adequate downsizing of CRC liver metastases to allow further treatment with LITT. The combined treatment illustrates substantial survival rates and high local tumour control with statistically significant differences between the three protocols used. Further randomised trials addressing the current study results are required.
评估在不可切除结直肠癌(CRC)肝转移患者中使用不同化疗方案进行多次经动脉化疗栓塞(TACE)缩瘤治疗,随后进行磁共振引导激光间质热疗(LITT)的治疗方案。
本研究共纳入 224 例患者。TACE(每位患者平均 3.4 次)作为缩小肿瘤的治疗方法,以满足 LITT 要求(数量≤5,直径<5cm)。动脉内方案包括伊立替康联合丝裂霉素(n=77)、吉西他滨联合丝裂霉素(n=49)或单独丝裂霉素(n=98),所有患者均使用碘油和 Embocept。TACE 后,所有患者均行 LITT(每位患者平均 2.2 次)。
总体而言,TACE 使靶病灶的平均直径缩小了 21.4%。从治疗开始计算的中位无进展时间为 8 个月,从治疗完成开始计算的中位局部肿瘤控制率为 7.5 个月。从 TACE 开始计算的患者中位总生存时间为 23 个月(范围 4-110 个月),伊立替康联合丝裂霉素组的中位总生存时间为 22.5 个月,吉西他滨联合丝裂霉素组为 23 个月,单独使用丝裂霉素组为 24 个月,三组间存在统计学差异(P<0.01)。
重复 TACE 可使 CRC 肝转移瘤充分缩小,以便进一步进行 LITT 治疗。三种方案联合治疗的结果显示,患者的生存率和局部肿瘤控制率较高,且三组间存在统计学差异。需要进一步开展随机试验来验证本研究结果。