Center for Human Nutrition and Atkins Center of Excellence in Obesity Medicine, Washington University School of Medicine, St. Louis, Missouri, USA.
Diabetes Care. 2012 Jun;35(6):1316-21. doi: 10.2337/dc11-1951. Epub 2012 Apr 3.
To provide a comprehensive assessment of multiorgan insulin sensitivity in lean and obese subjects with normal glucose tolerance.
The hyperinsulinemic-euglycemic clamp procedure with stable isotopically labeled tracer infusions was performed in 40 obese (BMI 36.2 ± 0.6 kg/m(2), mean ± SEM) and 26 lean (22.5 ± 0.3 kg/m(2)) subjects with normal glucose tolerance. Insulin was infused at different rates to achieve low, medium, and high physiological plasma concentrations.
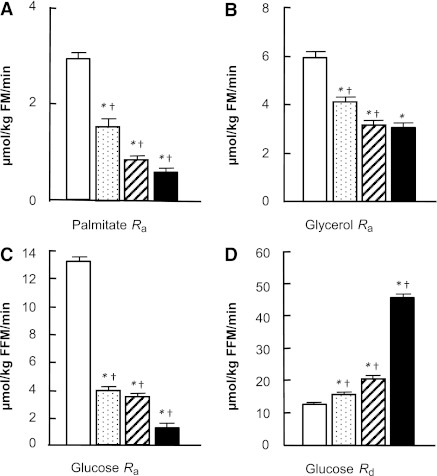
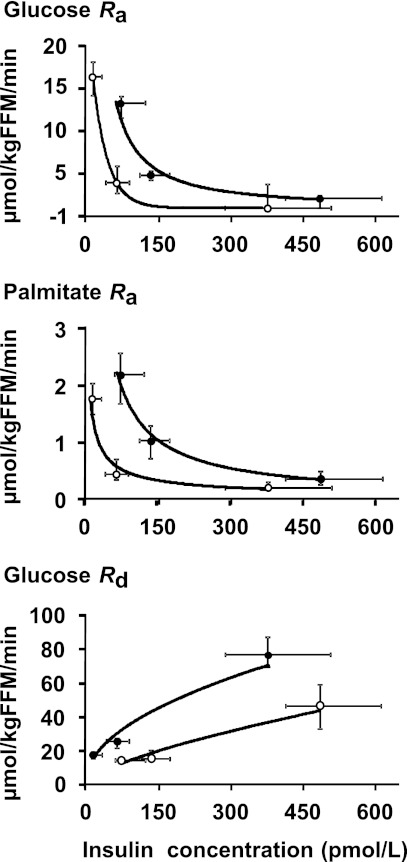
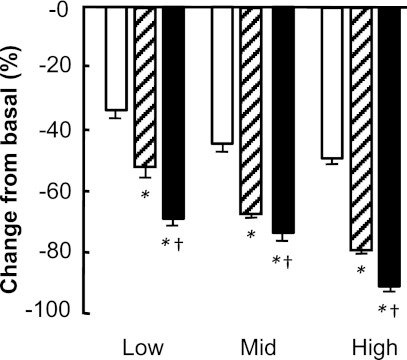
In obese subjects, palmitate and glucose R(a) in plasma decreased with increasing plasma insulin concentrations. The decrease in endogenous glucose R(a) was greater during low-, medium-, and high-dose insulin infusions (69 ± 2, 74 ± 2, and 90 ± 2%) than the suppression of palmitate R(a) (52 ± 4, 68 ± 1, and 79 ± 1%). Insulin-mediated increase in glucose disposal ranged from 24 ± 5% at low to 253 ± 19% at high physiological insulin concentrations. The suppression of palmitate R(a) and glucose R(a) were greater in lean than obese subjects during low-dose insulin infusion but were the same in both groups during high-dose insulin infusion, whereas stimulation of glucose R(d) was greater in lean than obese subjects across the entire physiological range of plasma insulin.
Endogenous glucose production and adipose tissue lipolytic rate are both very sensitive to small increases in circulating insulin, whereas stimulation of muscle glucose uptake is minimal until high physiological plasma insulin concentrations are reached. Hyperinsulinemia within the normal physiological range can compensate for both liver and adipose tissue insulin resistance, but not skeletal muscle insulin resistance, in obese people who have normal glucose tolerance.
全面评估糖耐量正常的瘦素抵抗和肥胖个体的多器官胰岛素敏感性。
对 40 例肥胖(BMI 36.2±0.6kg/m2,均值±SEM)和 26 例瘦素抵抗(22.5±0.3kg/m2)的糖耐量正常个体进行稳定同位素示踪剂输注的高胰岛素-正葡萄糖钳夹实验。以不同的速率输注胰岛素,以达到低、中、高生理血浆浓度。
在肥胖个体中,血浆棕榈酸和葡萄糖 R(a)随着血浆胰岛素浓度的增加而降低。在低、中、高剂量胰岛素输注期间,内源性葡萄糖 R(a)的降低幅度大于棕榈酸 R(a)的抑制幅度(69±2%、74±2%和 90±2%,52±4%、68±1%和 79±1%)。葡萄糖处置的胰岛素介导增加范围从低生理胰岛素浓度的 24±5%到高生理胰岛素浓度的 253±19%。在低剂量胰岛素输注期间,瘦素抵抗和肥胖个体的棕榈酸 R(a)和葡萄糖 R(a)抑制作用大于肥胖个体,但在高剂量胰岛素输注期间两组相同,而葡萄糖 R(d)刺激在整个生理胰岛素浓度范围内,瘦素抵抗个体大于肥胖个体。
内源性葡萄糖生成和脂肪组织脂肪分解率对循环胰岛素的微小增加都非常敏感,而肌肉葡萄糖摄取的刺激作用在达到高生理血浆胰岛素浓度之前是最小的。在糖耐量正常的肥胖个体中,正常生理范围内的高胰岛素血症可以补偿肝脏和脂肪组织的胰岛素抵抗,但不能补偿骨骼肌的胰岛素抵抗。