Department of Medicine, NYU Langone Medical Center, 550 First Avenue, New York, NY 10016, USA.
Comput Math Methods Med. 2012;2012:829465. doi: 10.1155/2012/829465. Epub 2012 Mar 15.
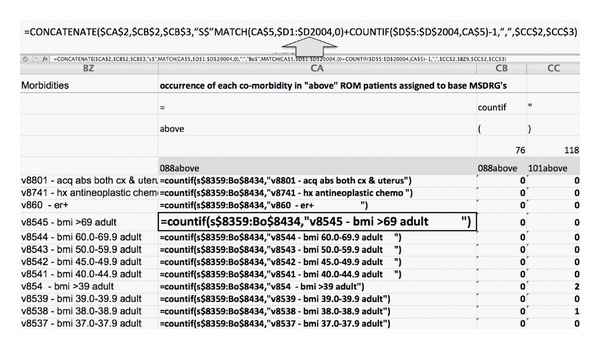
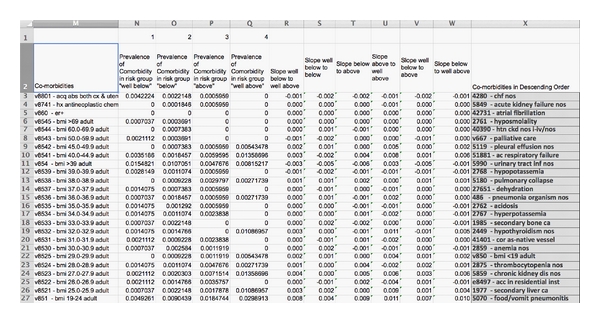
The ratio of observed-to-expected deaths is considered a measure of hospital quality and for this reason will soon become a basis for payment. However, there are drivers of that metric more potent than quality: most important are medical documentation and patient acuity. If hositals underdocument and therefore do not capture the full "expected mortality" they may be tempted to lower their observed/expected ratio by reducing "observed mortality" through limiting access to the very ill. Underdocumentation occurs because hospitals do not recognize, and therefore cannot seek to confirm, specific comorbidities conferring high mortality risk. To help hospitals identify these comorbidities, this paper describes an easily implemented spread-sheet for evaluating comorbid conditions associated, in any particular hospital, with each discharge. This method identifies comorbidities that increase in frequency as mortality risk increases within each diagnostic grouping. The method is inductive and therefore independent of any particular risk-adjustment technique.
观察到的与预期的死亡比例被认为是衡量医院质量的一个指标,因此很快将成为支付的基础。然而,有一些比质量更能驱动这一指标的因素:最重要的是医疗文件和患者的严重程度。如果医院记录不完整,因此无法完全捕捉到“预期死亡率”,他们可能会通过限制对非常病重的患者的治疗来降低观察到的/预期的死亡率。记录不完整是因为医院没有认识到(因此无法寻求确认)具体的合并症,这些合并症会带来高死亡率风险。为了帮助医院识别这些合并症,本文描述了一个易于实施的电子表格,用于评估与每个出院相关的、与特定医院相关的合并情况。该方法确定了在每个诊断分组中,随着死亡率风险的增加而频率增加的合并症。该方法是归纳性的,因此不依赖于任何特定的风险调整技术。