Department of Pediatrics and Communicable Diseases, University of Michigan Health System, Ann Arbor, Michigan 48109, USA.
BMC Pediatr. 2012 Jun 8;12:61. doi: 10.1186/1471-2431-12-61.
Child mortality in the United States has decreased over time, with advance in biomedicine. Little is known about patterns of current pediatric health care delivery for children with the leading causes of child death (high-impact conditions). We described patient and hospital characteristics, and hospital resource use, among children hospitalized with high-impact conditions, according to illness severity.
We conducted a retrospective study of children 0-18 years of age, hospitalized with discharge diagnoses of the ten leading causes of child death, excluding diagnoses not amenable to hospital care, using the 2006 version of the Kid's Inpatient Database. National estimates of average and cumulative hospital length of stay and total charges were compared between types of hospitals according to patient illness severity, which was measured using all-patient refined diagnosis related group severity classification into minor-moderate, major, and extreme severity.
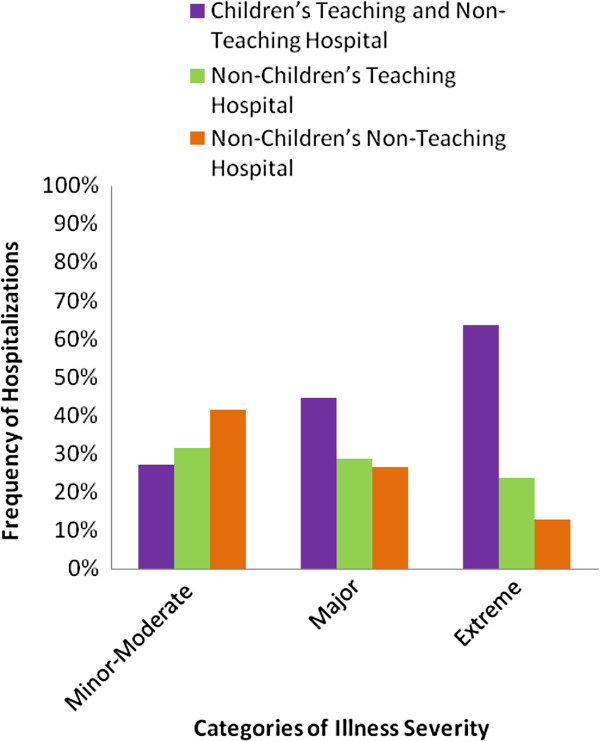
There were an estimated 3,084,548 child hospitalizations nationally for high-impact conditions in 2006, distributed evenly among hospital types. Most (84.4%) had minor-moderate illness severity, 12.2% major severity, and 3.4% were extremely ill. Most (64%) of the extremely ill were hospitalized at children's hospitals. Mean hospital stay was longest among the extremely ill (32.8 days), compared with major (9.8 days, p < 0.0001), or minor-moderate (3.4 days, p < 0.001) illness severity. Mean total hospital charges for the extremely ill were also significantly higher than for hospitalizations with major or minor-moderate severity. Among the extremely ill, more frequent hospitalization at children's hospitals resulted in higher annual cumulative charges among children's hospitals ($ 7.4 billion), compared with non-children teaching hospitals ($ 3.2 billion, p = 0.023), and non-children's non-teaching hospitals ($ 1.5 billion, p < 0.001). Cumulative annual length of hospital stay followed the same pattern, according to hospital type.
Gradation of increasing illness severity among children hospitalized for high-impact conditions was associated with concomitantly increased resource consumption. These findings have significant implications for children's hospitals which appear to accrue the highest resource use burden due to preferential hospitalization of the most severely ill at these hospitals.
随着生物医学的进步,美国儿童死亡率呈下降趋势。对于目前导致儿童死亡的主要原因(高影响力疾病)的儿科医疗服务模式,人们知之甚少。我们根据疾病严重程度,描述了患有高影响力疾病的住院儿童的患者和医院特征以及医院资源利用情况。
我们对 2006 年儿童住院数据库中的 0-18 岁儿童进行了回顾性研究,这些儿童的出院诊断为导致儿童死亡的十大主要原因,不包括无法进行医院治疗的诊断。根据所有患者精细诊断相关组严重程度分类,将患者的疾病严重程度分为轻度至中度、重度和极重度,对不同类型医院的平均和累计住院时间以及总费用进行了全国估计。
2006 年,全国范围内估计有 3084548 例儿童因高影响力疾病住院,分布在各类型医院之间。大多数(84.4%)疾病严重程度为轻度至中度,12.2%为重度,3.4%为极重度。极重度疾病的患者中,大多数(64%)在儿童医院住院。与重度(9.8 天,p<0.0001)或轻度至中度(3.4 天,p<0.001)疾病严重程度相比,极重度疾病患者的平均住院时间最长。极重度疾病患者的总住院费用也明显高于重度或轻度至中度疾病患者。在极重度疾病患者中,儿童医院的频繁住院导致儿童医院的年累计费用高于非儿童医院教学医院($74 亿美元)和非儿童医院非教学医院($15 亿美元,p<0.001)。根据医院类型,住院年累计时间也遵循相同的模式。
患有高影响力疾病住院的儿童的疾病严重程度逐渐加重,同时资源消耗也随之增加。这些发现对儿童医院具有重要意义,因为这些医院优先收治最严重的患儿,因此似乎承担了最高的资源利用负担。