Nestaas Eirik, Støylen Asbjørn, Fugelseth Drude
Department of Paediatrics, Vestfold Hospital Trust, Tønsberg, Norway.
BMJ Open. 2012 Aug 24;2(4). doi: 10.1136/bmjopen-2012-001636. Print 2012.
To investigate one-segment strain and strain rate indices as measures of myocardial performance in asphyxiated term neonates.
Quality improvement cohort study.
Newborns admitted to a neonatal intensive care unit at a Norwegian University Hospital for perinatal asphyxia and non-asphyxiated newborn recruited from the maternity ward at the same hospital.
Twenty asphyxiated and 48 non-asphyxiated term neonates.
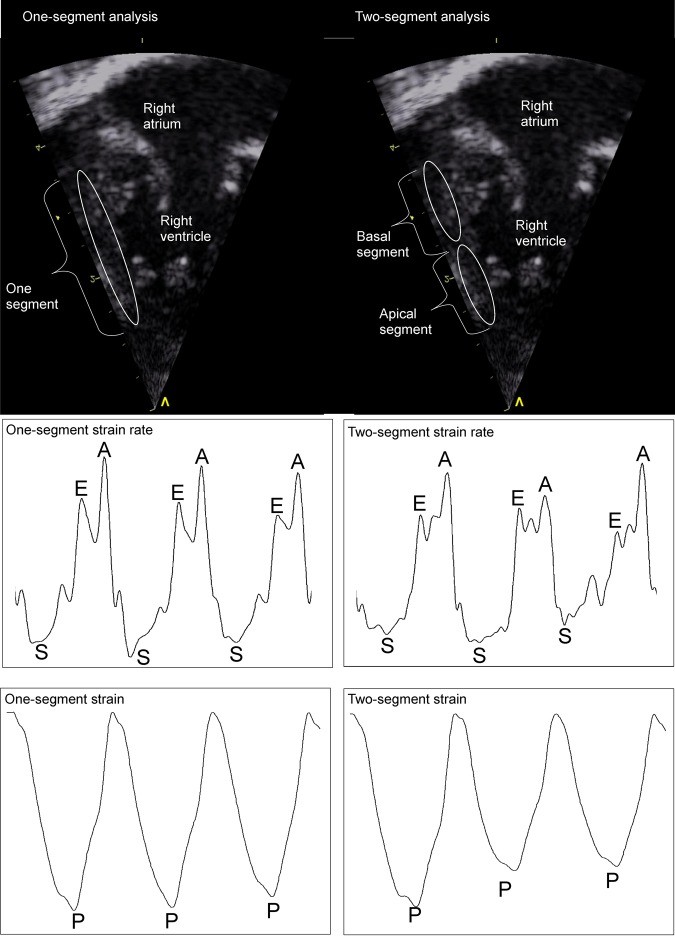
Strain and strain rate indices and repeatability measures. One-segment longitudinal strain and strain rate by tissue Doppler were assessed on days 1, 2 and 3 of life in nine heart walls. Repeatability was compared against measurements from two-segment analyses previously performed in the same images.
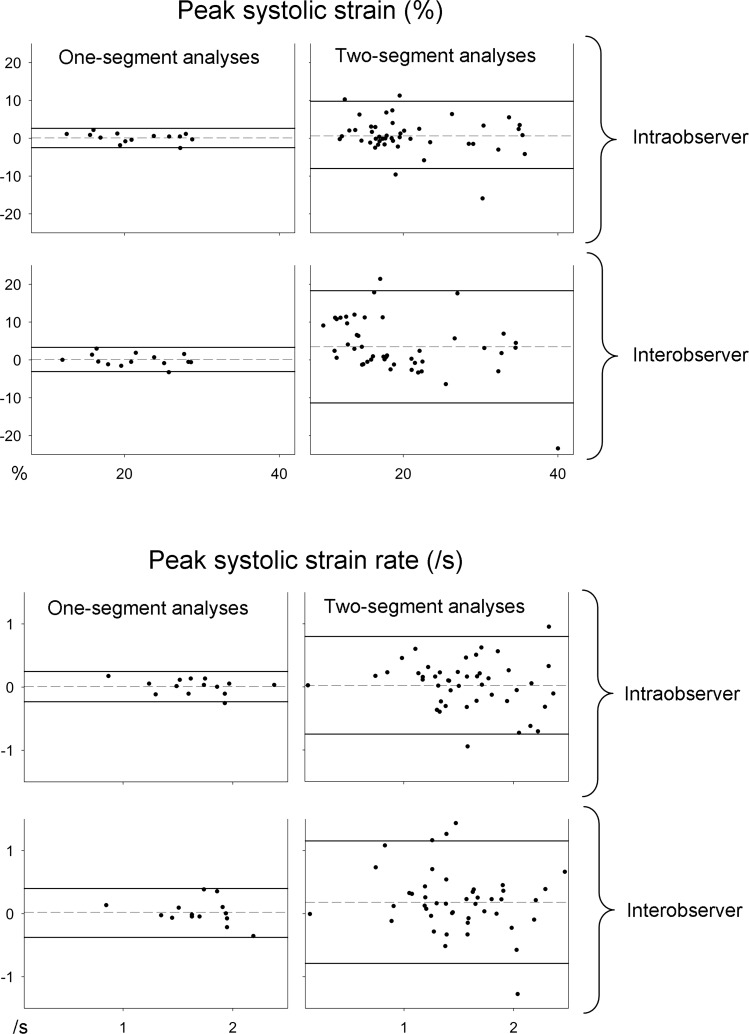
The 95% limits of agreement were significantly better for the one-segment than two-segment repeatability analyses, the inter-rater peak systolic strain (PSS) was (-3.1, 3.3) vs (-11.4, 18.3)%, the inter-rater peak systolic strain rate (PSSR) was (-0.38, 0.40) vs (-0.79, 1.15)/s, the intra-rater PSS was (-2.5, 2.6) vs (-8.0, 9.8)% and the intra-rater PSSR was (-0.23, 0.25) vs (-0.75, 0.80)/s (p<0.05). The myocardial performance was lower in the asphyxiated neonates (indices closer to zero) than in the non-asphyxiated neonates, PSS was -17.8 (0.6) (mean (SEM)) vs -21.2 (0.3)%, PSSR -1.43 (0.08) vs -1.61 (0.03)/s, early diastolic strain rate 1.72 (0.11) vs 2.00 (0.11)/s and strain rate during the atrial systole 1.92 (0.17) vs 2.27 (0.10)/s (p<0.05), despite no difference in fractional shortening (29.0 (0.5) vs 29.1 (1.0)%) (p>0.05).
One-segment strain and strain rate assessed the reduced myocardial performance in asphyxiated neonates with significantly improved reproducibility as compared with two-segment analysis and was therefore more feasible than two-segment analyses for assessment of myocardial performance after perinatal asphyxia.
研究单节段应变和应变率指标作为窒息足月儿心肌功能的测量方法。
质量改进队列研究。
挪威大学医院新生儿重症监护病房收治的因围产期窒息的新生儿,以及从同一家医院产科病房招募的非窒息新生儿。
20名窒息足月儿和48名非窒息足月儿。
应变和应变率指标以及重复性测量。在出生后第1、2和3天,对9个心壁采用组织多普勒评估单节段纵向应变和应变率。将重复性与之前在相同图像中进行的双节段分析测量结果进行比较。
单节段重复性分析的95%一致性界限明显优于双节段分析,评分者间的峰值收缩期应变(PSS)为(-3.1,3.3)% 对比(-11.4,18.3)%,评分者间的峰值收缩期应变率(PSSR)为(-0.38,0.40)/s对比(-0.79,1.15)/s,同一评分者的PSS为(-2.5,2.6)%对比(-8.0,9.8)%,同一评分者的PSSR为(-0.23,0.25)/s对比(-0.75,0.80)/s(p<0.05)。窒息新生儿的心肌功能低于非窒息新生儿(指标更接近零),PSS为-17.8(0.6)(均值(标准误))对比-21.2(0.3)%,PSSR为-1.43(0.08)对比-1.61(0.03)/s,舒张早期应变率为1.72(0.11)对比2.00(0.11)/s,心房收缩期应变率为1.92(0.17)对比2.27(0.10)/s(p<0.05),尽管缩短分数无差异(29.0(0.5)对比29.1(1.0)%)(p>0.05)。
与双节段分析相比,单节段应变和应变率可评估窒息新生儿心肌功能降低,且重复性显著提高,因此在评估围产期窒息后心肌功能方面比双节段分析更可行。