Kaiser Permanente Center for Health Research, Portland, OR, USA.
J Gen Intern Med. 2013 May;28(5):691-7. doi: 10.1007/s11606-012-2320-1. Epub 2013 Jan 24.
Cardiovascular disease (CVD) prevention in diabetes requires broad-based treatment of dyslipidemia, hypertension, and hyperglycemia. The independent contribution of all combinations of risk factor control to CVD risk has not been evaluated.
To estimate the independent association of control of glycosylated hemoglobin (A1C), systolic blood pressure (SBP), and low-density lipoprotein cholesterol (LDL-C) with risk of cardiovascular disease hospitalization.
Non-concurrent longitudinal cohort study.
The study included 26,636 patients with type 2 diabetes who were members of an integrated group model HMO with multiple A1C, SBP, and LDL-C measurements.
Patients were followed for a mean (SD) of 5.6 (2.5) years until they died or disenrolled, or until 31 December 2010. The outcome was a first-observed CVD hospitalization. Using the mean of all A1C, SBP, and LDL-C measures during follow-up, we created dichotomous categories of A1C control (< 7 %), SBP control (< 130 mmHg), and LDL-C control (< 100 mg/dL) to estimate the incidence rate of CVD hospitalization associated with all combinations of risk factor control adjusting for demographic and clinical characteristics.
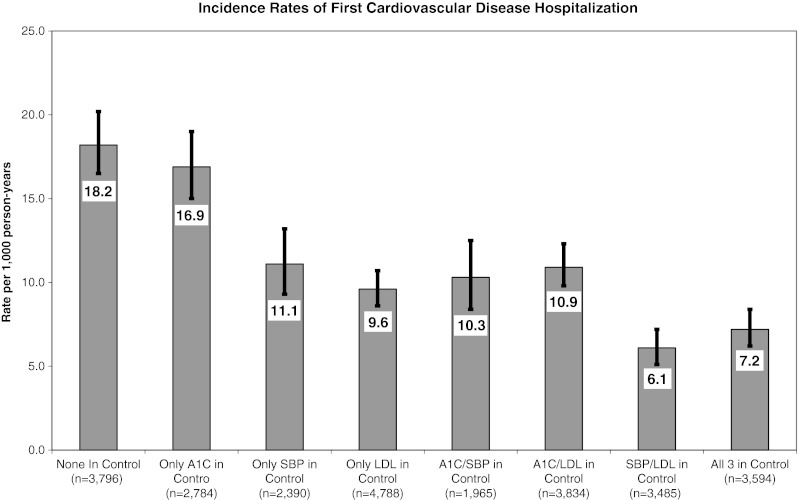
Patients with no controlled risk factors (18.2/1,000 person-years, 95 % CI 16.5-20.2) or with only A1C in control (16.9, 15.0-19.0) had the highest rate of CVD hospitalization, whereas those with all three risk factors controlled (7.2, 6.2-8.4) or with SBP and LDL-C in control (6.1, 5.1-7.2) had the lowest rates. Those with only SBP or LDL-C in control, A1C and SBP controlled, or A1C and LDL-C controlled had statistically similar incidence between the highest and lowest rates.
Maintaining SBP < 130 mmHg or LDL-C < 100 mg/dL was significantly associated with reduced CVD hospitalization risk, especially when both risk factors were well controlled. Maintaining A1C < 7 % was not independently associated with reduced CVD hospitalization risk.
糖尿病患者的心血管疾病(CVD)预防需要广泛治疗血脂异常、高血压和高血糖。尚未评估所有危险因素控制组合对 CVD 风险的独立贡献。
评估糖化血红蛋白(A1C)、收缩压(SBP)和低密度脂蛋白胆固醇(LDL-C)控制对心血管疾病住院风险的独立关联。
非同期纵向队列研究。
该研究纳入了 26636 名患有 2 型糖尿病的患者,他们是一家综合团体模式 HMO 的成员,该 HMO 有多次 A1C、SBP 和 LDL-C 测量值。
患者平均(标准差)随访 5.6(2.5)年,直至死亡、退出或截至 2010 年 12 月 31 日。结局是首次观察到的 CVD 住院。根据随访期间所有 A1C、SBP 和 LDL-C 测量值的平均值,我们创建了 A1C 控制(<7%)、SBP 控制(<130mmHg)和 LDL-C 控制(<100mg/dL)的二分类别,以估计在调整人口统计学和临床特征后,与所有危险因素控制组合相关的 CVD 住院发生率。
没有控制危险因素的患者(18.2/1000 人年,95%CI 16.5-20.2)或仅 A1C 控制的患者(16.9,15.0-19.0)的 CVD 住院率最高,而所有三种危险因素均得到控制的患者(7.2,6.2-8.4)或 SBP 和 LDL-C 得到控制的患者(6.1,5.1-7.2)的 CVD 住院率最低。仅 SBP 或 LDL-C 控制、A1C 和 SBP 控制或 A1C 和 LDL-C 控制的患者,其发病率介于最高和最低之间,差异无统计学意义。
保持 SBP<130mmHg 或 LDL-C<100mg/dL 与降低 CVD 住院风险显著相关,尤其是当两种危险因素都得到很好控制时。保持 A1C<7%与降低 CVD 住院风险无关。