Patnaik Ashis, Mishra Sudhansu Sekhar, Senapati Satya Bhushan, Patra Sunil Kalpalata, Tripathy Kalpalata, Burma Subrat
Department of Neurosurgery, SCB Medical College and Hospital, Cuttack, Odisha, India.
Surg Neurol Int. 2012;3:157. doi: 10.4103/2152-7806.105096. Epub 2012 Dec 26.
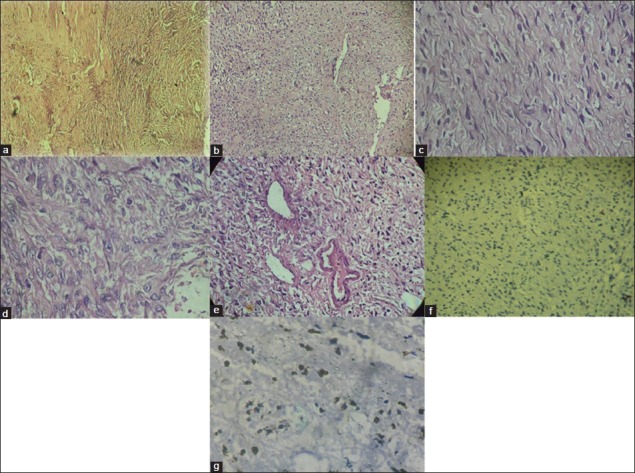
According to World Health Organization (WHO) classification of tumors, malignant peripheral nerve sheath tumors (MPNST) encompass the tumors, which were previously termed as malignant schwannoma, neurogenic sarcoma, and neurofibrosarcoma. These are rare tumors constituting only 5% of all malignant soft tissue tumors. As per their name, they arise from the malignant proliferation of cells forming sheath of a nerve root. They cause spinal cord compression, secondary changes in the surrounding bone with variable amount of tumor tissue going into the paraspinal space. However, purely intraosseous origin of the MPNST with no visible connection with a nerve root or dura is rare and few cases have been described in the literature.
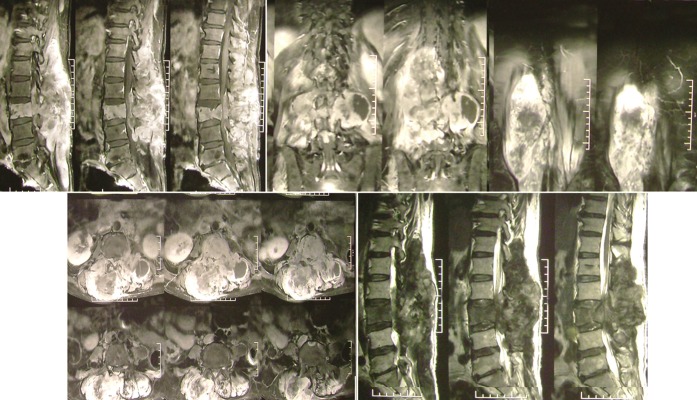
We present a primary intraosseous MPNST arising from the body of a thoracic spine with a minimal intraspinal component. However, there was a huge tumor part occupying the paraspinal and retrospinal region. The latter component was so large that it extended to lie just beneath the skin. The intraspinal component was confined to only one level. The giant extraspinal part was spanning multiple corresponding spinal level. We could not find such presentation in the literature.
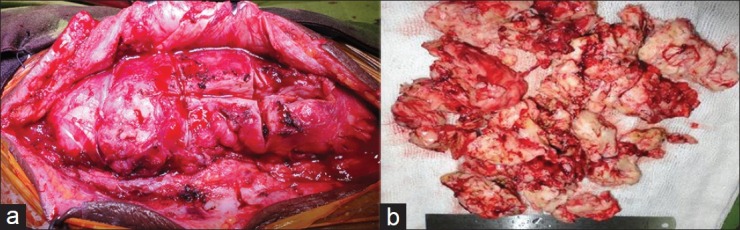
Gross total removal (GTR) followed by adjuvant chemo-radiotherapy is the optimal treatment for MPNST of spine. In case of multiple laminectomy or gross spinal instability, spinal instrumentation makes the treatment protocol complete.
根据世界卫生组织(WHO)的肿瘤分类,恶性外周神经鞘瘤(MPNST)包括以前被称为恶性神经鞘瘤、神经源性肉瘤和神经纤维肉瘤的肿瘤。这些是罕见的肿瘤,仅占所有恶性软组织肿瘤的5%。顾名思义,它们起源于形成神经根鞘的细胞的恶性增殖。它们会导致脊髓受压,周围骨骼发生继发性改变,并有不同数量的肿瘤组织进入椎旁间隙。然而,MPNST纯粹起源于骨内且与神经根或硬脑膜无明显连接的情况很少见,文献中仅有少数病例报道。
我们报告一例起源于胸椎椎体的原发性骨内MPNST,脊髓内成分极少。然而,有一个巨大的肿瘤部分占据了椎旁和椎后区域。后者部分非常大,一直延伸到皮肤下方。脊髓内成分仅局限于一个节段。巨大的椎外部分跨越了多个相应的脊柱节段。我们在文献中未发现此类病例。
对于脊柱MPNST,最佳治疗方法是行全切除(GTR),然后进行辅助放化疗。如果进行了多次椎板切除术或脊柱严重不稳定,则需进行脊柱内固定以使治疗方案完整。