Centre for Cardiovascular Genetics, British Heart Foundation Laboratories, Institute of Cardiovascular Science, Rayne Building University College London, London WC1E 6JF, UK.
Atherosclerosis. 2013 Jul;229(1):161-8. doi: 10.1016/j.atherosclerosis.2013.04.011. Epub 2013 Apr 18.
To determine the frequency and spectrum of mutations causing Familial Hypercholesterolaemia (FH) in patients attending a single UK specialist hospital lipid clinic in Oxford and to identify characteristics contributing to a high mutation detection rate.
289 patients (272 probands) were screened sequentially over a 2-year period for mutations in LDLR, APOB and PCSK9 using standard molecular genetic techniques. The Simon Broome (SB) clinical diagnostic criteria were used to classify patients and a separate cohort of 409 FH patients was used for replication.
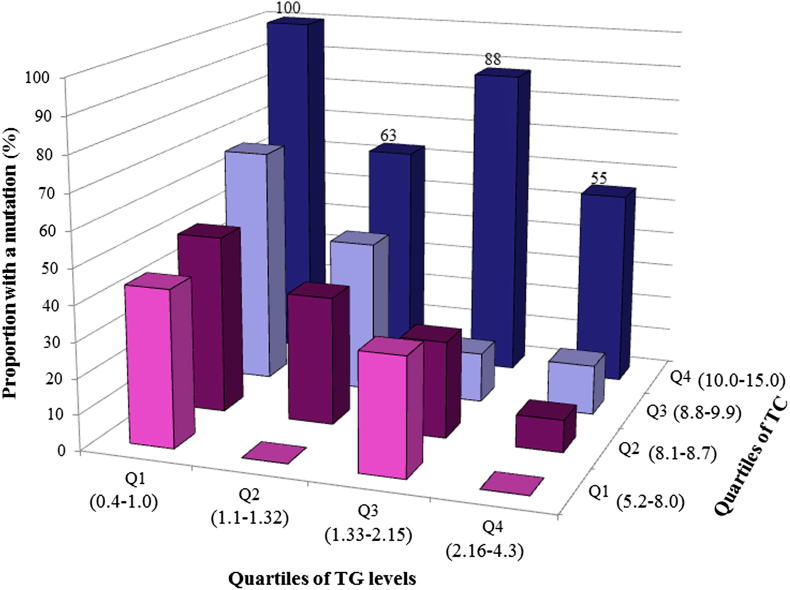
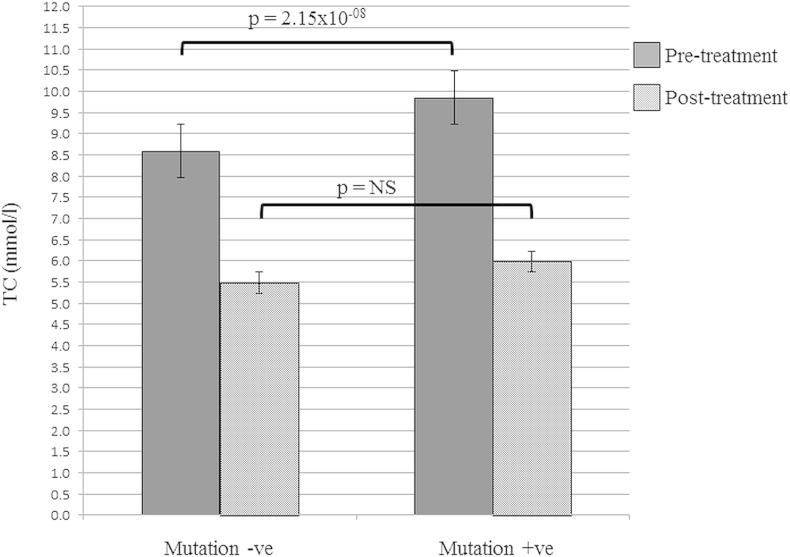
An FH-causing mutation was found in 101 unrelated patients (LDLR = 54 different mutations, APOB p.(Arg3527Gln) = 10, PCSK9 p.(Asp374Tyr) = 0). In the 60 SB Definite FH patients the mutation detection rate was 73% while in the 142 with Possible FH the rate was significantly lower (27%, p < 0.0001), but similar (14%, p = 0.06) to the 70 in whom there was insufficient data to make a clinical diagnosis. The mutation detection rate varied significantly (p = 9.83 × 10(-5)) by untreated total cholesterol (TC) levels (25% in those <8.1 mmol/l and 74% in those >10.0 mmol/l), and by triglyceride levels (20% in those >2.16 mmol/l and 60% in those <1.0 mmol/l (p = 0.0005)), with both effects confirmed in the replication sample (p for trend = 0.0001 and p = 1.8 × 10(-6) respectively). There was no difference in the specificity or sensitivity of the SB criteria versus the Dutch Lipid Clinic Network score in identifying mutation carriers (AROC respectively 0.73 and 0.72, p = 0.68).
In this genetically heterogeneous cohort of FH patients the mutation detection rate was significantly dependent on pre-treatment TC and triglyceride levels.
确定在牛津一家英国专科诊所脂质门诊就诊的家族性高胆固醇血症(FH)患者中导致 FH 的基因突变的频率和谱,并确定导致高突变检出率的特征。
在两年期间,使用标准分子遗传学技术对 289 名患者(272 名先证者)进行 LDLR、APOB 和 PCSK9 基因突变的连续筛查。使用 Simon Broome(SB)临床诊断标准对患者进行分类,并使用单独的 409 名 FH 患者队列进行验证。
在 101 名无血缘关系的患者中发现了 FH 致病突变(LDLR=54 种不同的突变,APOB p.(Arg3527Gln)=10,PCSK9 p.(Asp374Tyr)=0)。在 60 名 SB 明确 FH 患者中,突变检出率为 73%,而在 142 名可能 FH 患者中,突变检出率显著较低(27%,p<0.0001),但与无临床诊断数据的 70 名患者相似(14%,p=0.06)。突变检出率随未治疗的总胆固醇(TC)水平显著变化(p=9.83×10(-5))(8.1mmol/L 以下的患者为 25%,10.0mmol/L 以上的患者为 74%),随甘油三酯水平显著变化(2.16mmol/L 以上的患者为 20%,1.0mmol/L 以下的患者为 60%(p=0.0005)),在验证样本中均证实了这两种效应(趋势检验 p=0.0001,p=1.8×10(-6))。SB 标准与荷兰脂质诊所网络评分在识别突变携带者方面的特异性和敏感性无差异(分别为 AROC0.73 和 0.72,p=0.68)。
在该遗传异质性的 FH 患者队列中,突变检出率与治疗前 TC 和甘油三酯水平显著相关。