Department of Radiation Oncology, University of California San Francisco San Francisco, CA, USA.
Front Oncol. 2013 May 10;3:110. doi: 10.3389/fonc.2013.00110. eCollection 2013.
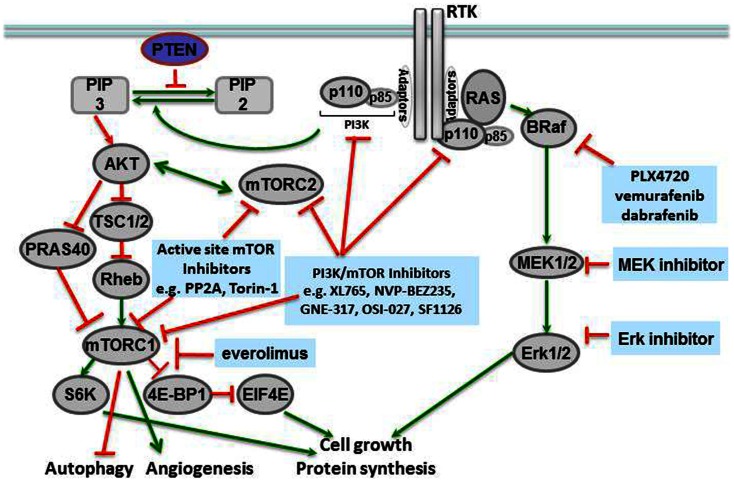
Brain tumors are the most common solid pediatric malignancy. For high-grade, recurrent, or refractory pediatric brain tumors, radiation therapy (XRT) is an integral treatment modality. In the era of personalized cancer therapy, molecularly targeted agents have been designed to inhibit pathways critical to tumorigenesis. Our evolving knowledge of genetic aberrations in pediatric gliomas is being exploited with the use of specific targeted inhibitors. These agents are additionally being combined with XRT to increase the efficacy and duration of local control. In this review, we discuss novel agents targeting three different pathways in gliomas, and their potential combination with XRT. BRAF is a serine/threonine kinase in the RAS/RAF/MAPK kinase pathway, which is integral to cellular division, survival, and metabolism. Two-thirds of pilocytic astrocytomas, a low-grade pediatric glioma, contain a translocation within the BRAF gene called KIAA1549:BRAF that causes an overactivation of the MEK/MAPK signaling cascade. In vitro and in vivo data support the use of MEK or mammalian target of rapamycin (mTOR) inhibitors in low-grade gliomas expressing this translocation. Additionally, 15-20% of high-grade pediatric gliomas express BRAF V600E, an activating mutation of the BRAF gene. Pre-clinical in vivo and in vitro data in BRAF V600E gliomas demonstrate dramatic cooperation between XRT and small molecule inhibitors of BRAF V600E. Another major signaling cascade that plays a role in pediatric glioma pathogenesis is the PI3-kinase (PI3K)/mTOR pathway, known to be upregulated in the majority of high- and low-grade pediatric gliomas. Dual PI3K/mTOR inhibitors are in clinical trials for adult high-grade gliomas and are poised to enter studies of pediatric tumors. Finally, many brain tumors express potent stimulators of angiogenesis that render them refractory to treatment. An analog of thalidomide, CC-5103 increases the secretion of critical cytokines of the tumor microenvironment, including IL-2, IFN-γ, TNF-α, and IL-10, and is currently being evaluated in clinical trials for the treatment of recurrent or refractory pediatric central nervous system tumors. In summary, several targeted inhibitors with radiation are currently under investigation in both translational bench research and early clinical trials. This review article summarizes the molecular rationale for, and the pre-clinical data supporting the combinations of these targeted agents with other anti-cancer agents and XRT in pediatric gliomas. In many cases, parallels are drawn to molecular mechanisms and targeted inhibitors of adult gliomas. We additionally discuss the potential mechanisms underlying the efficacy of these agents.
脑肿瘤是最常见的儿童实体恶性肿瘤。对于高级别、复发性或难治性儿童脑肿瘤,放射治疗(XRT)是一种重要的治疗方式。在个性化癌症治疗时代,已经设计了分子靶向药物来抑制肿瘤发生的关键途径。我们对儿童神经胶质瘤遗传异常的不断认识正在通过使用特定的靶向抑制剂来利用。这些药物还与 XRT 联合使用,以提高局部控制的疗效和持续时间。在这篇综述中,我们讨论了靶向神经胶质瘤中三种不同途径的新型药物及其与 XRT 的潜在联合应用。BRAF 是 RAS/RAF/MAPK 激酶途径中的丝氨酸/苏氨酸激酶,对细胞分裂、存活和代谢至关重要。三分之二的毛细胞型星形细胞瘤是一种低级别儿童神经胶质瘤,在 BRAF 基因内存在称为 KIAA1549:BRAF 的易位,导致 MEK/MAPK 信号级联的过度激活。体外和体内数据支持在表达这种易位的低级别神经胶质瘤中使用 MEK 或哺乳动物雷帕霉素靶蛋白(mTOR)抑制剂。此外,15-20%的高级别儿童神经胶质瘤表达 BRAF V600E,这是 BRAF 基因的一种激活突变。BRAF V600E 神经胶质瘤的临床前体内和体外数据表明,XRT 与 BRAF V600E 的小分子抑制剂之间存在显著的协同作用。另一个在儿童神经胶质瘤发病机制中起作用的主要信号通路是 PI3-激酶(PI3K)/mTOR 通路,该通路在大多数高级别和低级别儿童神经胶质瘤中上调。双重 PI3K/mTOR 抑制剂正在进行成人高级别神经胶质瘤的临床试验,并准备进入儿科肿瘤的研究。最后,许多脑肿瘤表达强烈的血管生成刺激因子,使其对治疗产生抗性。沙利度胺类似物 CC-5103 增加了肿瘤微环境中关键细胞因子的分泌,包括 IL-2、IFN-γ、TNF-α 和 IL-10,目前正在临床试验中评估用于治疗复发性或难治性儿童中枢神经系统肿瘤。总之,目前正在进行转化基础研究和早期临床试验,以研究几种与辐射相结合的靶向抑制剂。本文综述了这些靶向药物与其他抗癌药物和 XRT 联合应用于儿童神经胶质瘤的分子基础和临床前数据。在许多情况下,与成人神经胶质瘤的分子机制和靶向抑制剂进行了类比。我们还讨论了这些药物疗效的潜在机制。