Renal-Electrolyte Division, Department of Medicine, University of Pittsburgh, Pittsburgh, Pa., USA.
Am J Nephrol. 2013;38(6):489-95. doi: 10.1159/000356939. Epub 2013 Dec 10.
Fatigue is an important symptom to patients with advanced chronic kidney disease (CKD). The aim of this study is to examine the prevalence and severity of fatigue among non-dialysis-dependent CKD and end-stage renal disease (ESRD) patients, to examine the association of fatigue with subjective and objective sleep quality, and to identify other modifiable factors associated with fatigue.
A cross-sectional survey of 87 non-dialysis-dependent CKD (eGFR ≤45 ml/min/1.73 m(2)) and 86 ESRD patients was done using the Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-F) and 36-Item Short-Form (SF-36) vitality scale. Higher FACIT-F score denoted less fatigue. Objective sleep was assessed using in-home polysomnography. Predictors of fatigue were determined using a linear regression model.
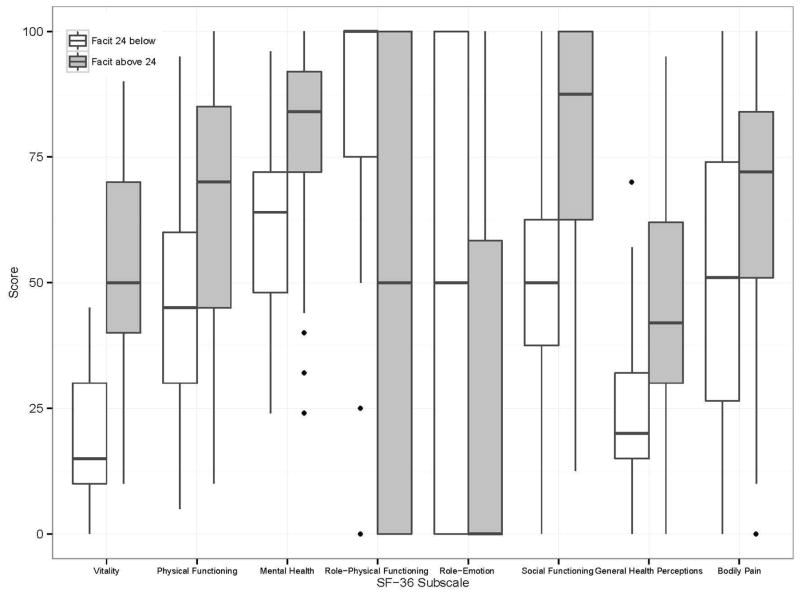
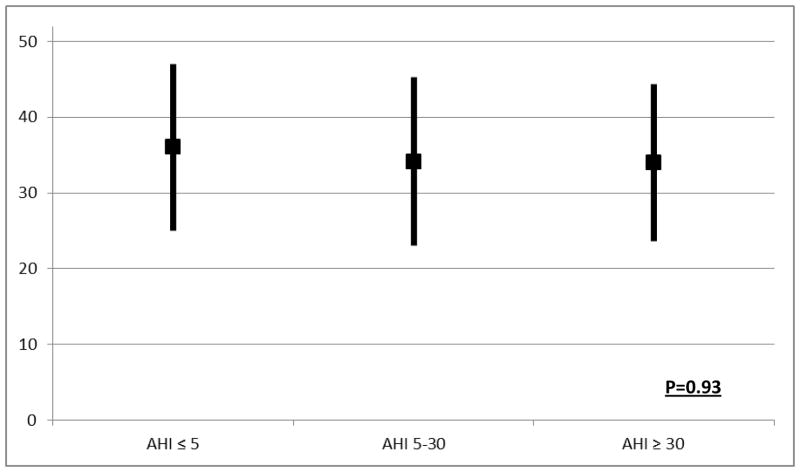
The mean FACIT-F score among all participants was 34.5 ± 11.0. Mean scores were similar among CKD and ESRD groups (34.25 ± 11.28 vs. 34.73 ± 10.86; p = 0.73). On univariate analyses, patients with higher levels of fatigue were more likely to have cardiovascular disease, benzodiazepine use, depressive symptoms, and slightly lower hemoglobin and serum albumin levels. There was no significant association between severity of sleep apnea and level of fatigue (Apnea Hypopnea Index 20.1 ± 27.6 vs. 20.3 ± 22.0; p = 0.69). Presence of cardiovascular disease, low serum albumin, depressive symptoms, poor subjective sleep quality, excessive daytime sleepiness and restless legs syndrome were independently associated with greater fatigue in multivariable regression models. The FACIT-F score correlated closely with the SF-36 vitality score (r = 0.81, p < 0.0001).
Patients with advanced CKD and ESRD experience profound fatigue. Depressive symptoms, restless legs syndrome, excessive daytime sleepiness, and low albumin levels may provide targets for interventions to improve fatigue in patients with advanced CKD.
疲劳是晚期慢性肾脏病(CKD)患者的一个重要症状。本研究旨在检查非透析依赖性 CKD 和终末期肾病(ESRD)患者疲劳的患病率和严重程度,检查疲劳与主观和客观睡眠质量的关系,并确定与疲劳相关的其他可改变的因素。
采用慢性疾病治疗功能评估-疲劳量表(FACIT-F)和 36 项简明健康调查问卷(SF-36)活力量表对 87 名非透析依赖性 CKD(eGFR ≤45 ml/min/1.73 m²)和 86 名 ESRD 患者进行横断面调查。较高的 FACIT-F 评分表示疲劳程度较低。使用家庭多导睡眠图评估客观睡眠。使用线性回归模型确定疲劳的预测因素。
所有参与者的平均 FACIT-F 得分为 34.5 ± 11.0。CKD 和 ESRD 组的平均得分相似(34.25 ± 11.28 vs. 34.73 ± 10.86;p = 0.73)。在单变量分析中,疲劳程度较高的患者更有可能患有心血管疾病、使用苯二氮䓬类药物、出现抑郁症状,且血红蛋白和血清白蛋白水平略低。严重睡眠呼吸暂停与疲劳程度之间无显著相关性(呼吸暂停低通气指数 20.1 ± 27.6 vs. 20.3 ± 22.0;p = 0.69)。心血管疾病、低血清白蛋白、抑郁症状、较差的主观睡眠质量、白天过度嗜睡和不宁腿综合征是多变量回归模型中与疲劳程度增加相关的独立因素。FACIT-F 评分与 SF-36 活力评分密切相关(r = 0.81,p < 0.0001)。
晚期 CKD 和 ESRD 患者会经历严重的疲劳。抑郁症状、不宁腿综合征、白天过度嗜睡和低白蛋白血症可能为改善晚期 CKD 患者的疲劳提供干预靶点。