de Biase Dario, Visani Michela, Malapelle Umberto, Simonato Francesca, Cesari Valentina, Bellevicine Claudio, Pession Annalisa, Troncone Giancarlo, Fassina Ambrogio, Tallini Giovanni
Department of Medicine (DIMES) - Anatomic Pathology Unit, Bellaria Hospital, University of Bologna, Bologna, Italy.
Department of Pharmacology and Biotechnology (FaBiT), University of Bologna, Bologna, Italy.
PLoS One. 2013 Dec 23;8(12):e83607. doi: 10.1371/journal.pone.0083607. eCollection 2013.
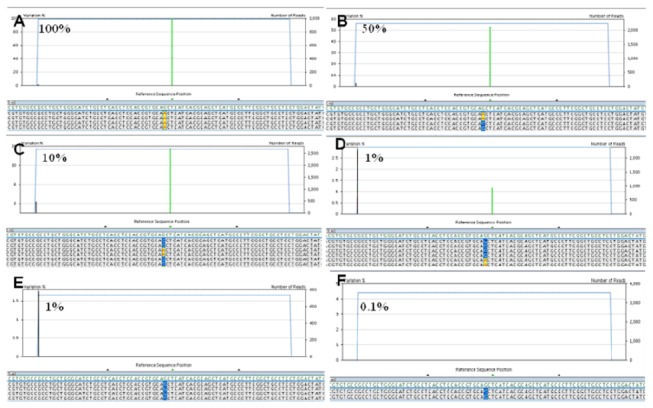
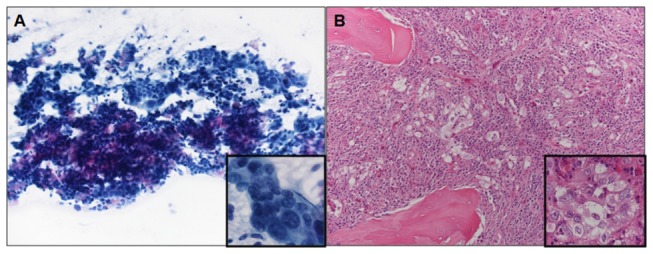
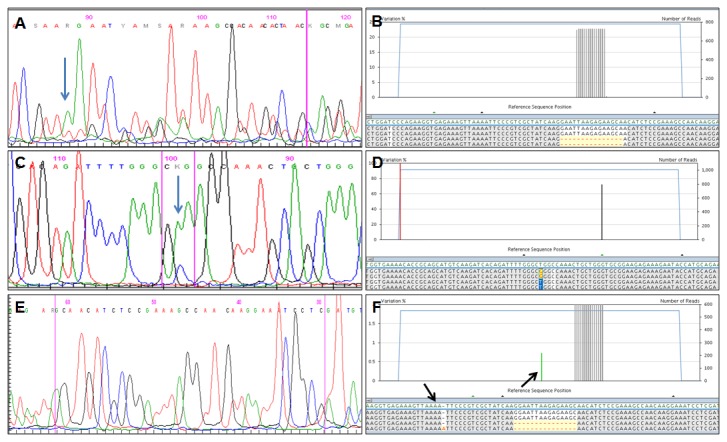
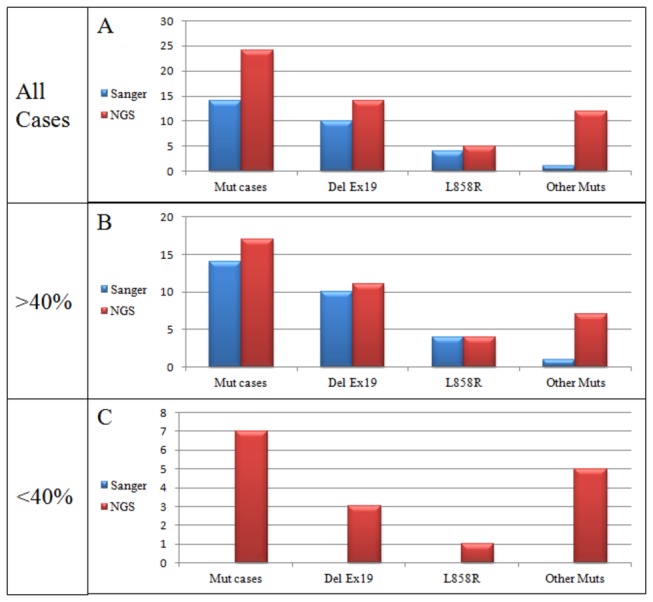
Selection of lung cancer patients for therapy with tyrosine kinase inhibitors directed at EGFR requires the identification of specific EGFR mutations. In most patients with advanced, inoperable lung carcinoma limited tumor samples often represent the only material available for both histologic typing and molecular analysis. We defined a next generation sequencing protocol targeted to EGFR exons 18-21 suitable for the routine diagnosis of such clinical samples. The protocol was validated in an unselected series of 80 small biopsies (n=14) and cytology (n=66) specimens representative of the material ordinarily submitted for diagnostic evaluation to three referral medical centers in Italy. Specimens were systematically evaluated for tumor cell number and proportion relative to non-neoplastic cells. They were analyzed in batches of 100-150 amplicons per run, reaching an analytical sensitivity of 1% and obtaining an adequate number of reads, to cover all exons on all samples analyzed. Next generation sequencing was compared with Sanger sequencing. The latter identified 15 EGFR mutations in 14/80 cases (17.5%) but did not detected mutations when the proportion of neoplastic cells was below 40%. Next generation sequencing identified 31 EGFR mutations in 24/80 cases (30.0%). Mutations were detected with a proportion of neoplastic cells as low as 5%. All mutations identified by the Sanger method were confirmed. In 6 cases next generation sequencing identified exon 19 deletions or the L858R mutation not seen after Sanger sequencing, allowing the patient to be treated with tyrosine kinase inhibitors. In one additional case the R831H mutation associated with treatment resistance was identified in an EGFR wild type tumor after Sanger sequencing. Next generation sequencing is robust, cost-effective and greatly improves the detection of EGFR mutations. Its use should be promoted for the clinical diagnosis of mutations in specimens with unfavorable tumor cell content.
选择肺癌患者接受针对表皮生长因子受体(EGFR)的酪氨酸激酶抑制剂治疗,需要识别特定的EGFR突变。在大多数晚期、无法手术的肺癌患者中,有限的肿瘤样本通常是进行组织学分型和分子分析的唯一可用材料。我们定义了一种针对EGFR第18至21外显子的新一代测序方案,适用于对此类临床样本进行常规诊断。该方案在意大利三个转诊医疗中心未经选择的80例小活检(n = 14)和细胞学(n = 66)标本系列中得到验证,这些标本代表了通常提交用于诊断评估的材料。系统评估标本中肿瘤细胞数量以及相对于非肿瘤细胞的比例。每次运行以100 - 150个扩增子为一批进行分析,分析灵敏度达到1%,并获得足够数量的读数,以覆盖所有分析样本的所有外显子。将新一代测序与桑格测序进行比较。后者在14/80例(17.5%)中鉴定出15个EGFR突变,但当肿瘤细胞比例低于40%时未检测到突变。新一代测序在24/80例(30.0%)中鉴定出31个EGFR突变。在肿瘤细胞比例低至5%时也能检测到突变。桑格法鉴定出的所有突变均得到证实。在6例中,新一代测序鉴定出桑格测序后未发现的第19外显子缺失或L858R突变,使患者能够接受酪氨酸激酶抑制剂治疗。在另外1例中,桑格测序后在EGFR野生型肿瘤中鉴定出与治疗耐药相关的R831H突变。新一代测序稳健、具有成本效益,并且大大提高了EGFR突变的检测率。对于肿瘤细胞含量不利的标本中突变的临床诊断,应推广使用该方法。